Obesity is an important public health problem in children and adolescent because of the rapid increase in its prevalence rate and its related co-morbidities.
To estimate the prevalence of overweight and obesity among intermediate school student in Buraydah, aged from 13 to 16 years and to discover the associated risk factors.
A cross-sectional study was carried out in a government school in Buraydah, during academic year 2018-2019. All the study population were subjected to a predesigned questionnaire that included questions related to socio-demographic characteristics, life style (physical activity and eating habits) and anthropometric measurements including height, weight and body mass index.
216 students participated in this study. The prevalence of overweight and obesity was 24.1% and 10.1% respectively. The highest rate of overweight was at the age of 13-14 years. Risk factors of obesity were intake of breakfast and snacks, fast food consumption, > 2 hours per day of screen watching, eating while watching television and low level of physical activity.
This study found a relatively high prevalence of overweight and obesity among intermediate school's students, aged 13-16 years in Buraydah. Risk factors of overweight and obesity were, harmful feeding habits and physical inactivity.
Prevalence, Overweight, Obesity, Body mass index, Dietary habits, Lifecycle
Obesity has emerged as an epidemic in many parts of the world. The World Health Organization has warned of the escalating epidemic of obesity that could put the population in many countries at risk of developing non-communicable diseases. Available studies in Eastern Mediterranean countries indicate that obesity has reached an alarming level among both children and adults. Consequently, the incidence of non-communicable diseases is also very high, and represents more than 50% of total causes of death [1]. According to National Health and Nutrition Examination Survey (2011-2014), childhood obesity rates have remained stable for the past decade at around 17 percent for ages 2 to 19. However, these rates are declining among 2 to 5-year-olds, stable among 6 to 11-year-olds, and increasing among 12- to 19-year-olds [2].
The mechanism of obesity development is not fully understood and it is confirmed that obesity occurs when energy intake exceeds energy expenditure. There are multiple etiologies for this imbalance; hence, the rising prevalence of obesity cannot be addressed by a single etiology. Genetic factors influence the susceptibility of a given child to an obesity conducive environment. However, environmental factors, lifestyle preferences, and cultural environment seem to play major roles in the rising prevalence of obesity worldwide [3,4]. In a small number of cases, childhood obesity is due to genes such as leptin deficiency or medical causes such as hypothyroidism and growth hormone deficiency or side effects due to drugs (e.g. steroids) [1].
Overweight and obesity lead to adverse metabolic effects on blood pressure, cholesterol, triglycerides and insulin resistance. Some confusion of the consequences of obesity arise because researchers have used different BMI cut-offs, and because the presence of many medical conditions involved in the development of obesity may confuse the effects of obesity itself. The non-fatal, but debilitating health problems associated with obesity include respiratory difficulties, chronic musculoskeletal problems, skin problems and infertility. The more life-threatening problems fall into four main areas such as CVD problems; conditions associated with insulin resistance such as type 2 diabetes; certain types of cancers, especially the hormonally related and large-bowel cancers; and gallbladder disease [3].
In Saudi Arabia, there is an increasing trend in the prevalence of obesity and overweight, which are the sources of various diseases including hypertension, diabetes, obstructive sleep apnea, CVD etc.
This study focused on prevalence of overweight and obesity among intermediate schools students in Buraydah, KSA.
A cross-sectional study was conducted on a sample of students who attended government schools during the second school academic term. The sampling frame included the listed governmental schools given by Educational Directorate of boridah.
Buraidah is the capital of the Emirate of Qassim in the Kingdom of Saudi Arabia and the largest city of Qassim with a population of over half a million. Buraidah surrounds a range of hills and sandy highlands, including some depressions, which are very fertile agricultural lands because of the easy extraction of water from its surface covered with a layer of limestone and gypsum. It is warm in summer, cold in winter and relatively humid. It dominated by northerly winds that reduce heat in the summer and northeasterly, which works to reduce heat in the winter. The area of Buraidah is currently estimated at about 1,300 square kilometers. The city is famous for agriculture and many farms that produce dates and has a global market for dates trading, where all kinds of dates and is an important place come to the Arabs to buy dates specifically.
The population of this study was all students aged 13- 16-years-old in all schools in Buraiadh Educational Directorates. A cluster random sampling was used. A list of public schools was obtained from the education directorates and clusters were created for each of the Directorate and two schools were selected randomly from each cluster. Finally, three classes from each school were selected randomly.
Two schools were used to collect data for this study. The total sample size was 216 participants aged 13-16 years, based on the following formula: N = [(1.96)2 × pq]/d2, where N = sample size, p = expected prevalence, q = 1-p, d = margin of error. To calculate the 95% confidence interval for an expected prevalence of 25% (based on the average percentage prevalence of overweight and obesity in the world) with a margin of error (d) of not more than 0.03, the required sample size was 800. To cover for nonparticipation, we enlarged the sample as follows:
N = (1.96)2 × (0.25) × (1-0.25)/(0.25)2 = 216
After obtaining permission from heads of educational directorates, the researcher visited the selected schools to inform them about the survey. All the classes from the first to the third grade in each selected school were included in the study. Systematic randomization was used to select the sample where the students in the middle three desks from each row in each class were selected to give them the consent form (which was approved by the Regional Ethics Committee. Having got the consent from the headmasters and the students, data were collected by using the following tools.
Questionnaire: The contents of the predesigned questionnaire were explained to the students before handling over to them. The questionnaire included items like:
(A) Socio-demographic characteristics such as age, grade, gender, birth date, school name, residence, parents' educational level [illiterate, read and writing (elementary), school (upto high school), university], occupation of father [unskilled workers, skilled workers, semi-professional, professional], occupation of mother [working or not working], family size and numbers of houserooms.
(B) Feeding pattern: Data included the frequency of breakfast intake in a week، and number of meals، eating snacks and fast food consumption.
(C) Life style factors included: 1. Hours of television watching and computer/video games were recorded for each day of a typical week and divided into three time categories, such as no television watching, 62 h per day, > 2 h per day.
2. Eating while television watching.
3. A questionnaire on physical activity was developed by asking the participants to recall the number of hours per week if they had participated in any structured physical activity or team sport in the last six months. The participants were also asked about the time spent in commuting between home and school. Physical activity were divided into three time categories, such as no physical activity (less than 10 min per day), sometimes (10-30 min per day) and frequent (more than 30 min per day).
Anthropometric measurements: The researcher personally took different anthropometric measurements at the examination room. Body mass index: It was calculated by dividing weight in kg by square height in meters.
Data were checked, entered and statistically analyzed by SPSS (Statistical Package for Social Sciences version 15).
Data on BMI showed that 24.1% of the total population sample was underweight, 47.7% normal weight, 18.1% overweight and 10.1% obese. Thus, the overall prevalence of overweight and obesity among these students was 28.2% (Figure 1).
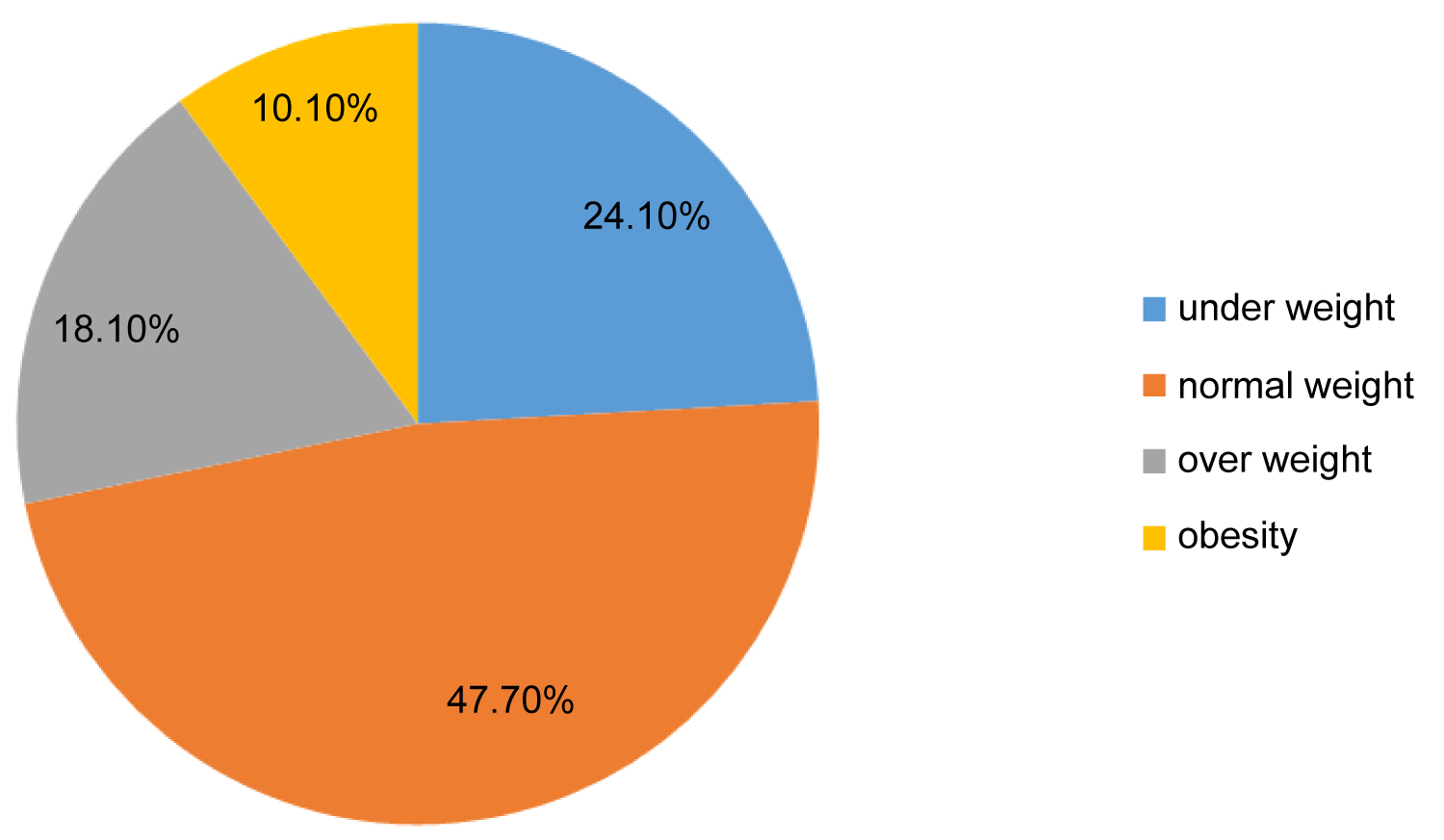 Figure 1: Prevalence of underweight, normal weight, overweight and obesity of middle schools student (n = 216).
View Figure 1
Figure 1: Prevalence of underweight, normal weight, overweight and obesity of middle schools student (n = 216).
View Figure 1
Of the 216 who participated, 45.8% were aged less than 14 years, wile (0.9%) only starting from the age of 16-years-old and above. About 61% of their parents 'educational level is above high school, while about a quarter of their parents' level of education is lower than above high school.
About one-third of the sample (30.0%) reported having a low family income, 46.8% middle income and 23.6% high income. The children's reports of their parents'education level showed that 16.2% of fathers and 25.5% of mothers had an educational level below high school, while 61.6% of the fathers and 55.6% of the mothers had above high-school education. Majority of the fathers had jobs (86.6%) while only 33.3% of the mothers had jobs (Table 1).
Table 1: Demographic characteristics of the samples of middle school's students (n = 216). View Table 1
Table 2 presents some of the important dietary habits of students in Buraydah. More than half of them (50.2%) reported of taking breakfast sometimes, whereas only 5.1% of them reported that they never took any breakfast. About daily numbers of meals, study showed that above half of respondents (53.7%) were taking three times meal a day. While quarter of them were taken above and less than three time. 73.6% of students, had taken snacks meals sometimes, while 21.3% had taken it in a frequency.
Table 2: Dietary habits of students (n = 216). View Table 2
The study demonstrated that more than fifty percent of middle school students have their nutritional behavior towards eating some food and beverages like fast food consumption, sweets intake, carbonated drinking intake and sweet juices drinking, (76.4%, 54.2%, 53.7%, 65.7%) respectively, and they do not tend to eat it permanently or more than once a day while sometimes they do so.While fresh vegetables and fruits were taken irregularly by 46.3% of the students.
Our data displayed that 45.5% of students were watching television more than 2 hours a day. In addition, more than two thirds (67.1%) of the students participating in the study, hadspent more time sitting in front of TV screens and telephones, and eat during this period. The study also shows that two third (65.3%) of students used their private cars to go to school (Table 3).
Table 3: Lifestyle factors of students (n = 216). View Table 3
Several variables were tested to determine their effect on BMI. The variables included dietary habits, associated with underweight, normal, overweight and obesity, which are shown in Table 4. Our data showed a significant association between breakfast intake, daily snack meals and fast food consumption lead to a higher BMI respectively, (p value < 0.005, p value < 0.004 and p value < 0.000), while having more fresh fruits and vegetables, carbonated drinking intake and juices drinking were not significantly associated with BMI, (p value < 0.008, p value < 0.032 and p value < 0.351).
Table 4: Dietary habits associated with underweight, normal, overweight and obesity in the studied school adolescents. View Table 4
In Table 5 different variables were tested to determine their effect on BMI including life style factors. Data showed thatspending more time in front of the television and phone screens with eating foods and drinks regularly during this period and using private cars for transportation to school without enough exercisewere strongly significance associated with razing prevalence of overweight and obesity respectively (P value < 0.001, (P value < 0.000).
Table 5: Life style factor associated with underweight, normal, overweight and obesity in the studied school adolescents. View Table 5
Overweight and obesity is considered as an epidemic in many developed and developing countries of the world. The prevalence varies greatly by age group, sex and socioeconomic status [5]. In the present study, the overall prevalence of overweight and obesity in this sample of middle school students aged 13- 16-years-old was 28.2%. (24.1% overweight and 10.1% obese). In comparison to similar studies conducted in Saudi Arabia at different regions, our findings showed a higher prevalence of overweight than that observed in Jeddah 13.4% [6], Riyadh 13.8% [7]. These higher rates could be explained by low educational level of parents, unhealthy dietary behaviors with high caloric intake particularly snacks and fast food and life style of the participants. The prevalence of obesity also showed a lower rate than an intermediate schools study conducted in the Al-Medina with overall prevalence of overweight 16% and obesity 20.3% among male student aged between 12-15 years [8]. The prevalence of overweight and obesity in our study is higher other countries, where the overall prevalence of overweight and obesity among adolescents. For instance, the rate was 5.82% in Iran, 9.3% in Egypt, 10.4% in china, [9]. The prevalence rate of overweight and obesity in our study is almost similar to the result by Al Saeed, et al., [10] who discovered that the prevalence of overweight and obesity was 20% and 11% respectively [11], and Abdul-Aziz, [12] who revealed that the prevalence of overweight and obesity was 16% and 11% respectively. This difference might be attributed to the use of a different definition of obesity, or due to a gradual increase in the prevalence of obesity among adolescents since that time.
In the present study, there was a significant association exists between obesity and breakfast intake (p value < 0.005). This could be explained as increasing breakfast intakes of eating energy-dense, less-nutritious snacks and fast foods during the school hours, this agrees with Guven, et al., [13] study which exposed that the obese adolescents choose energy dense food. This study showed a significant association between obesity and snack intake (p value < 0.004) due to high fat and sugar content in snack foods. This is in line with several studies which found a significant relation between BMI and eating snack [14,15]. Also the present study revealed a significant association between obesity and more frequent fast food consumption (p value < 0.000), due to its high fat and calories. This is in agreement with the study conducted by Jerffey, et al. [15] who found a significant relation between BMI and fast food. While having more fresh fruits and vegetables, carbonated drinking intake and juices drinking were not significantly associated with BMI, (p value < 0.008, p value < 0.032 and p value < 0.351).
In the present study, there was a significant association between obesity and excessive use of computer and phone. Viewing computer and phone screens decreases energy disbursement, spending less time on performing physical activity and increases their consumption of obesogenic foods. This is in agreement with the study conducted by Munakata, et al., [16] who confirmed a significant relation between BMI and TV watching in Japan. Our study revealed a significant association with mode of transport for reaching school and obesity. Using own cars to reach school often devoid students of the benefit from walking on foot, physical exercises and energy consumption, which are in agreement with the findings of study by Souza [17].
The prevalence of overweight and obesity among intermediate schools, aged 13-16 years in Buraiyda was relatively high. Breakfast intake, snack intake, fast food consumption. Use of computer and phone, more than two hours per day, and finally physical inactivity showed a strong association with a higher BMI in the students.