To evaluate the clinical usefulness of the flexible fiberscope performed by two surgeons in patients with difficult laryngeal exposure.
This was a cross-sectional retrospective study, based on the analysis of 35 medical records of patients who underwent phonomicrosurgery for benign lesions of vocal cord between the years of 2015 and 2018.
Out of these patients, 3 patients presented with difficult laryngeal exposure that were operated under suspension microlaryngoscopy. Laryngeal exposure was much improved by the flexible fiberscope with a video system compared with the suspension microlaryngoscopy. The endolaryngeal surgeries in all cases with difficult laryngeal exposure were performed smoothly.
The flexible fiberscope with a video system could remarkably improve visualization of the larynx. This approach provided an alternative way for managing difficult laryngeal exposure during suspension microlaryngoscopy in phonomicrosurgery by two surgeons, without requirement of any specially designed instruments.
Difficult laryngeal exposure, The flexible fiberscope
Endolaryngeal microsurgery using a direct laryngoscope was a well-established procedure in phonosurgery [1]. Difficult laryngeal exposure during suspension microlaryngoscopic surgeries was not an uncommon situation encountered by the phonosurgeons [2]. Low exposure of the larynx could make laryngeal microsurgery difficult or even impossible [3]. Difficult laryngeal exposure might lead to unnecessary trauma, incomplete surgery and even abortion of the procedure [2].
There were numerous literatures discussing about prediction of difficult laryngeal exposure during suspension microlaryngoscopic surgeries. Thyroid-mandible angle might be a sensitive, reliable, and useful predictor of difficult laryngeal exposure in both men and women [4]. Patients with obesity, a muscular neck, or retrognathia were likely to present difficult laryngeal exposure, and preoperative measurement of these predictors might be useful in preparing for microlaryngosurgery [5]. Besides, the Laryngoscore might be a good predictor of difficult laryngeal exposure and assist in selecting the ideal candidates for operative microlaryngoscopy [6,7].
It was reported that various technique had been used for approaching difficult laryngeal exposure. Patient posture was one of the most important components in achieving ideal laryngeal exposure. The best posture for laryngeal exposure was believed to be the sniffing (Boyce-Jackson) position, with neck flexion and head extension [1]. External laryngeal counterpressure applied force directed posteriorly on the cricoid and lower thyroid cartilages, and helped the surgeon sufficiently view the anterior commissure of the vocal folds [1].
Besides, application of rigid endoscopy with angled instruments promoted full visualization of the surgical lesion and operative resolution [2,3]. Special scope had also been used for approaching difficult laryngeal exposure. It was reported that Airtraq® laryngoscope could remarkably improve visualization of the larynx and might provide an alternative way for managing difficult laryngeal exposure [8].
However, there was no report discussing using the flexible fiberscope with a video system for management of difficult laryngeal exposure during suspension microlaryngoscopy while patient receiving general anaesthesia [9]. The aim of this study was to evaluate the clinical usefulness of the flexible fiberscope with a video system in patients with difficult laryngeal exposure.
This was a cross-sectional retrospective study, based on the analysis of 35 medical records of patients who underwent phonomicrosurgery for benign lesions of vocal cord between the years of 2015 and 2018.
Out of these patients, 3 patients presented with difficult laryngeal exposure that were operated under suspension microlaryngoscopy using readily available flexible fiberscope along with a video system and microlaryngoscopic instruments, without requirement of any specially designed instruments. After suspension microlaryngoscopy was set up, the first surgeon held the flexible fiberscope and inserted the fiberscope into the suspension microlaryngoscopy. By using the fiberscope with a video system, this surgeon inspected the vocal lesion especially the anterior vocal area which was hard to be seen under traditional suspension microlaryngoscopy. The second surgeon then completed excision of vocal lesion with the microlaryngoscopic instruments by seeing the video system under control of the first surgeon.
Laryngeal exposure was much improved by the flexible fiberscope with a video system compared with the suspension microlaryngoscopy. Under the improved visualization of the larynx by the flexible fiberscope with a video system, the endolaryngeal surgeries in all cases with difficult laryngeal exposure were performed smoothly.
A 26-year-old male presented with bilateral vocal polyps for 2 years. This patient presented with difficult laryngeal exposure that were operated under suspension microlaryngoscopy using the flexible fiberscope along with a video system and microlaryngoscopic instruments (Figure 1 and Figure 2). By using the fiberscope with a video system, the first surgeon inspected the vocal lesion especially the anterior vocal area which was hard to be seen under traditional suspension microlaryngoscopy (Figure 3). The second surgeon performed excision of vocal lesion with the microlaryngoscopic instruments by seeing the video system (Figure 4).
 Figure 1: Under suspension microlaryngoscopy using the flexible fiberscope along with a video system.
View Figure 1
Figure 1: Under suspension microlaryngoscopy using the flexible fiberscope along with a video system.
View Figure 1
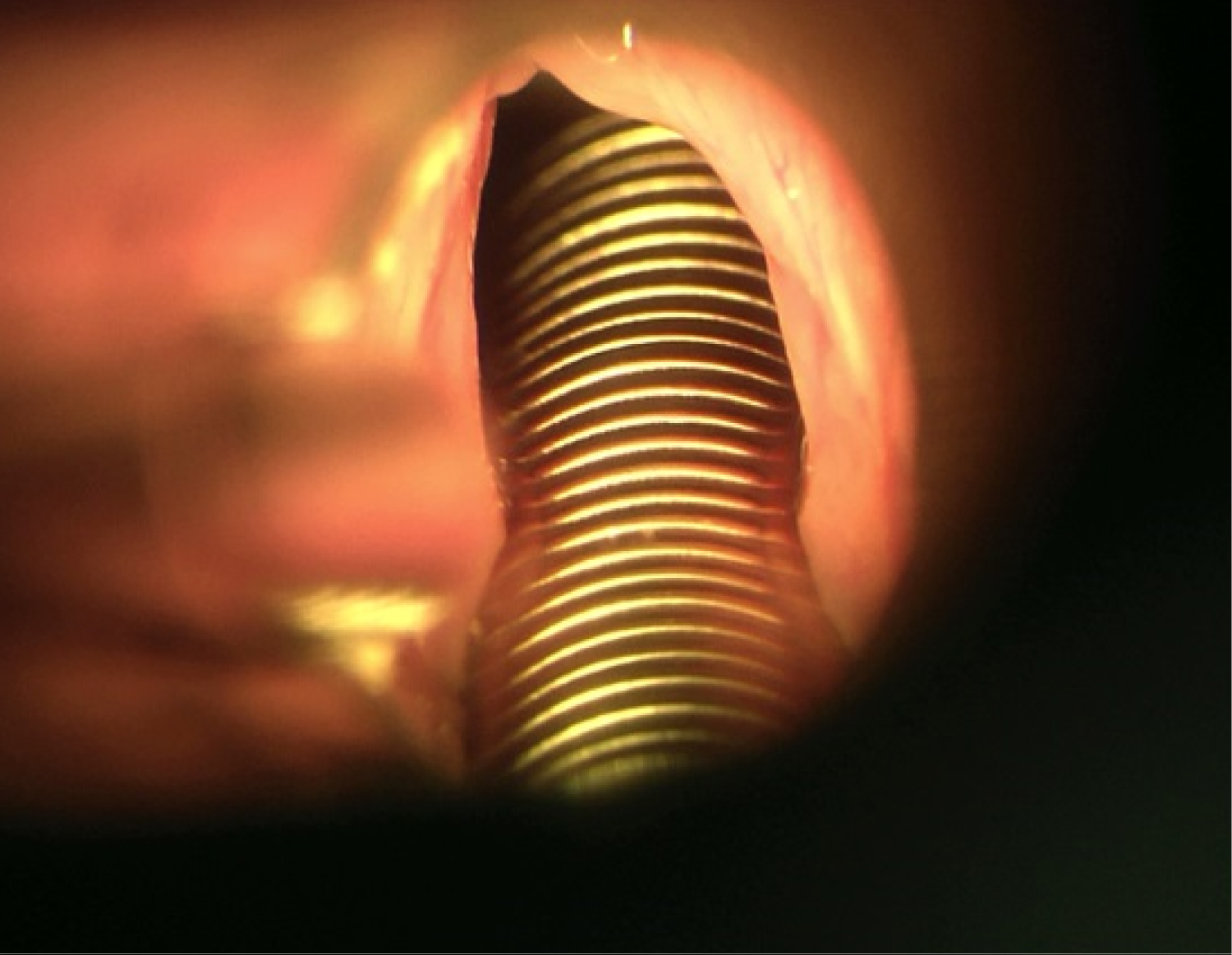 Figure 2: Presented with difficult laryngeal exposure that were operated under suspension microlaryngoscopy.
View Figure 2
Figure 2: Presented with difficult laryngeal exposure that were operated under suspension microlaryngoscopy.
View Figure 2
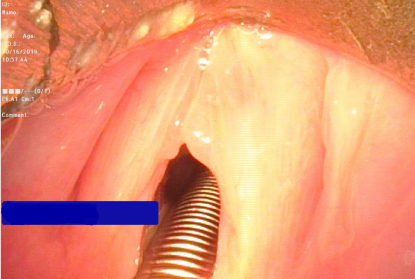 Figure 3: The fiberscope with a video system, the first surgeon inspected the vocal lesion especially the anterior vocal area which was hard to be seen under traditional suspension microlaryngoscopy.
View Figure 3
Figure 3: The fiberscope with a video system, the first surgeon inspected the vocal lesion especially the anterior vocal area which was hard to be seen under traditional suspension microlaryngoscopy.
View Figure 3
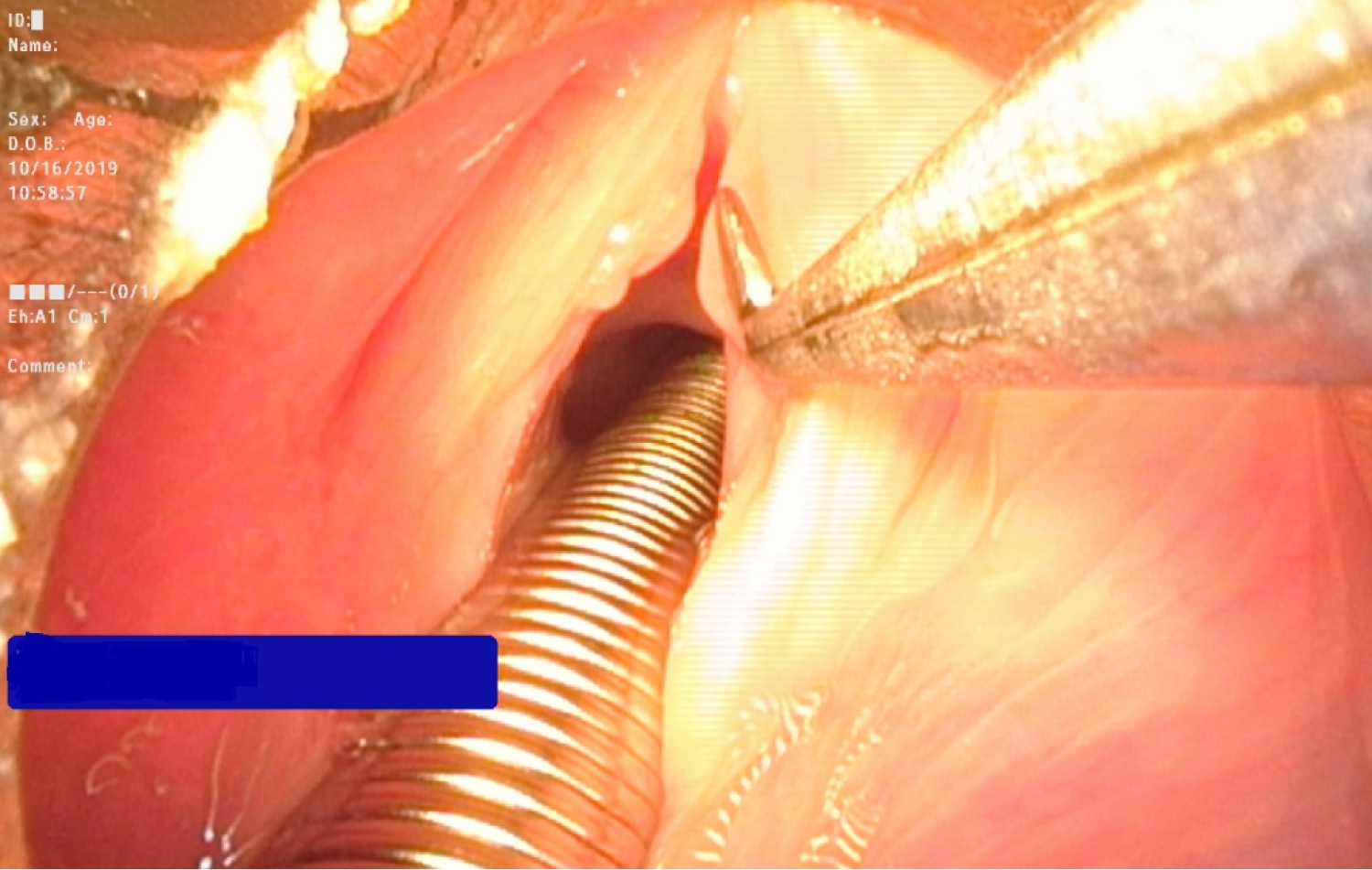 Figure 4: Performed excision of vocal lesion with the microlaryngoscopic instruments by seeing the video system.
View Figure 4
Figure 4: Performed excision of vocal lesion with the microlaryngoscopic instruments by seeing the video system.
View Figure 4
Otolaryngologists might inevitably encounter difficult laryngeal exposure in phonomicrosurgery [8]. Difficult laryngeal exposure might lead to unnecessary trauma, incomplete surgery and even abortion of the procedure [2]. Application of rigid endoscopy with angled instruments promoted full visualization of the surgical lesion and operative resolution [2,3]. It was reported that Airtraq® laryngoscope could remarkably improve visualization of the larynx and might provide an alternative way for managing difficult laryngeal exposure [8]. It was reported that with local anaesthesia, fiberoptic laryngeal surgery with topical anaesthesia was an another way for approaching difficult laryngeal exposure [1]. However, with general anaesthesia, there is no report discussing using flexible fiberscope with a video system for management of difficult laryngeal exposure during suspension microlaryngoscopy.
In our approach, we only needed the original endolaryngeal microsurgery instruments with the aid of the flexible fiberscope with a video system. We did not need other special surgical scopes or other special surgical instruments. This approach provided an alternative way for managing difficult laryngeal exposure during suspension microlaryngoscopy, especially when the hospital did not have the long angled rigid endoscopes designed for endolaryngeal microsurgery or when the hospital did not have the special surgical scope such as Airtraq® laryngoscope.
However, it was hard for a surgeon to hold the flexible fiberscope stably while simultaneously holding the endolaryngeal microsurgery instrument for doing the vocal surgery. Therefore, in our approach, there should be two surgeons to perform the operation. One surgeon hold the flexible fiberscope stably while the other surgeon hold the endolaryngeal microsurgery instructment doing the vocal surgery. The surgeon who hold the flexible fiberscope should better be an experienced surgeon in endolaryngeal microsurgery. An experienced surgeon who hold the flexible fiberscope would cooperate well with the other surgeon who hold the endolaryngeal microsurgery instructment doing the vocal surgery. Besides, while we were doing the suspension microlaryngoscopy with the flexible fiberscope, there was fog in the flexible fiberscope view initially. The fog would disappear in a few minutes.
The flexible fiberscope with a video system could remarkably improve visualization of the larynx. This approach provided an alternative way for managing difficult laryngeal exposure during suspension microlaryngoscopy in phonomicrosurgery by two surgeons, without requirement of any specially designed instruments.
None declared.
None declared.