Unsafe abortion was recognized problem worldwide which accounts 7.9% and 10% of all maternal mortality in the world and Ethiopia respectively. Nearly all unsafe abortions (98%) occur in developing countries. Even though the abortion penal code of Ethiopia was amended in 2005, to permit safe abortion under a set of some criteria, there is high number of unsafe abortion rate nationally (28/1000) and among University students (65/1000), from which only 50% was safe abortion which may be due to the possibility of low knowledge on liberalized safe abortion in our country.
To assess knowledge of safe abortion and associated factors among female students in Debre Markos University, Amhara Regional State, Northwest Ethiopia, April, 2016.
A cross sectional study was conducted on 483 undergraduate regular female students from April 4-18, 2016 in Debre Markos University. Simple random sampling was used. Self-administered structured questionnaire was used to collect data. Data was entered in to Epi Info version 7 and analyzed by SPSS version 20. Odds ratio with 95% confidence interval was used to identify associated factors and multivariable logistic regression to adjust the effects of possible cofounders.
All questionnaires (507) were filled, but 24 questionnaires were incomplete and have been rejected from the data analysis, which gives response rate of 95.3%. 199 (41.2%) of the respondents were knowledgeable about liberalized safe abortion. By multivariable logistic regression analysis, marital status [AOR = 2.44, 95% of CI:(1.35,4.42) ], family residence [AOR = 1.56, 95% of CI:(1.03, 2.39)], maternal educational level [AOR = 2.68, 95% of CI:(1.08,6.61)] and ever had pregnant before [AOR = 10.68, 95% of CI:(4.52,25.22)] were the factors significantly associated with knowledge of female students to liberalized safe abortion.
High proportions of students were not knowledgeable about safe abortion. Awareness creation toward safe abortion is very important in university students.
Knowledge, Safe abortion, Debre Markos University, Female students, Ethiopia
AOR: Adjusted Odds Ratio; BSc: Bachelor of Science; CI: Confidence Interval; COR: Crude Odds Ratio; DMU: Debre Markos University; MPH: Masters of Public Health; MSc: Masters of Science; OR: Odds Ratio; PAC: Post Abortion Care; RH: Reproductive Health; SPSS: Statistical Package for Social Sciences; WHO: World Health Organization
Abortion is the termination of pregnancy from the uterus before 20 weeks according to world health organization (WHO) or before 28 weeks (Ethiopia) gestational age, or in the absence of accurate dating criteria, born weighing < 500g. Abortion occurs spontaneously because of complication during pregnancy or it may be induced. WHO's definition of unsafe abortion was terminating an unintended pregnancy performed by person lacking the standardized skills and in a place that does not fulfilled minimal medical standards, or both [1,2].
Globally, unsafe abortions covers about 47,000 maternal mortality annually (13% of total maternal mortality) and contribute to significant morbidity among women, especially in low income settings [3]. About 30% of maternal mortality is because of unsafe abortion in Ghana [4]. Unsafe abortions include those abortion performed by untrained personnel under unhygienic conditions, those that are self-induced by a woman inserting a foreign object into her uterus or by consuming toxic products, and those initiated by physical trauma to a woman's abdomen [5,6].
Women die from unsafe abortion usually by severe infections, bleeding form problem of procedure or organ damage. Nearly half of all abortions in the world are done in unsafe condition, and nearly all unsafe abortions (98%) performed in developing countries [3,7]. Unsafe abortion has significant negative impacts in addition to its immediate effects on women's health. Unsafe abortion may reduce women's productivity, increasing the economic burden on poor families; cause maternal mortality which leave children motherless; result in long-term maternal health problems, like infertility and result in considerable costs burden to the public health systems [8]. In Ethiopia, the national rate of abortion was (28/1000 women aged 15-49) [9] and in Wolaita Sodo University students the abortion rate was 65 per 1000 women [10].
In Ethiopia unmarried adolescents are not supported to use contraceptives. This is cultural belief of our society which resulted in unintended under aged pregnancy. Due to lack awareness about safe abortion adolescents seek unsafe abortion in an undisclosed place. Study conducted in SNNPR Gedeo zone, Knowledge about the liberalized safe abortion law accounts for 48.21% [11] and same study in Harari regional state on female students revealed only 35.7% knows about safe abortion law [12].
Before 2005, abortion was permitted for the sake of saving maternal life in Ethiopia. In 2005, the abortion penal code was amended to allow abortion under a much wider set of criteria. Abortion is permitted before the fetus is viable (conventionally interpreted as 28 weeks after the last menstrual period) if (I) the pregnancy as a resulted of rape or incest, (II) if the pregnancy endanger the life of mother or baby, (III) the fetus has incurable and serious deformity, (IV) the woman has physical or mental disabilities or (V) the woman is a minor and is unprepared to raise a child [13,14].
Most of developing countries like Ethiopia, access to safe abortion was based on women's knowledge of the legal issue of safe abortion. Even though the 2005 Ethiopian abortion law is relatively liberal, but there is still high number of unsafe abortion as study done on students. So the knowledge of University students towards safe abortion is under question. There was limited literature which is published on knowledge of safe abortion among university students in Ethiopia. Therefore, this study assessed the knowledge of safe abortion and associated factors among undergraduate female students in Debre Markos University. So this study finding will be an input for other researchers for further studies on related issues, for planners and for stakeholders to fill the identified gaps.
Cross-sectional quantitative study has been conducted on institution from April 4-18, 2016 in Debre Markos University. The University runs undergraduate programs in both regular and continuing education divisions in six Colleges and one school with 34 departments. The university accommodated 12,807 regular students in which 3,508 were females in 2015/16 academic year. The University accommodated 772 academic staff, 58 assistant workers and 710 permanent administrative workers totally 1,540 up to the end of September 2015.
All regular undergraduate female students in Debre Markos University from selected colleges were study population. Students who were critically ill and those students on clinical attachment or field work which is far from campus during data collection were excluded. The sample size was determined by using single population proportion based on the proportion of awareness rate about liberalized safe abortion among female students attending college and university in Arba Minch town which is 32.1%, 4% precision, 95% confident level, 10% none response rate and used correction formula (n = n/1+n/N) [15]. With this assumptions sample of 507 female undergraduate regular female students from selected colleges were involved in the study. By using simple random sampling techniques four colleges were selected from seven colleges. List of female students were obtained from all departments of selected colleges and the required sample were allocated proportionally for all batches of students in that department (Figure 1).
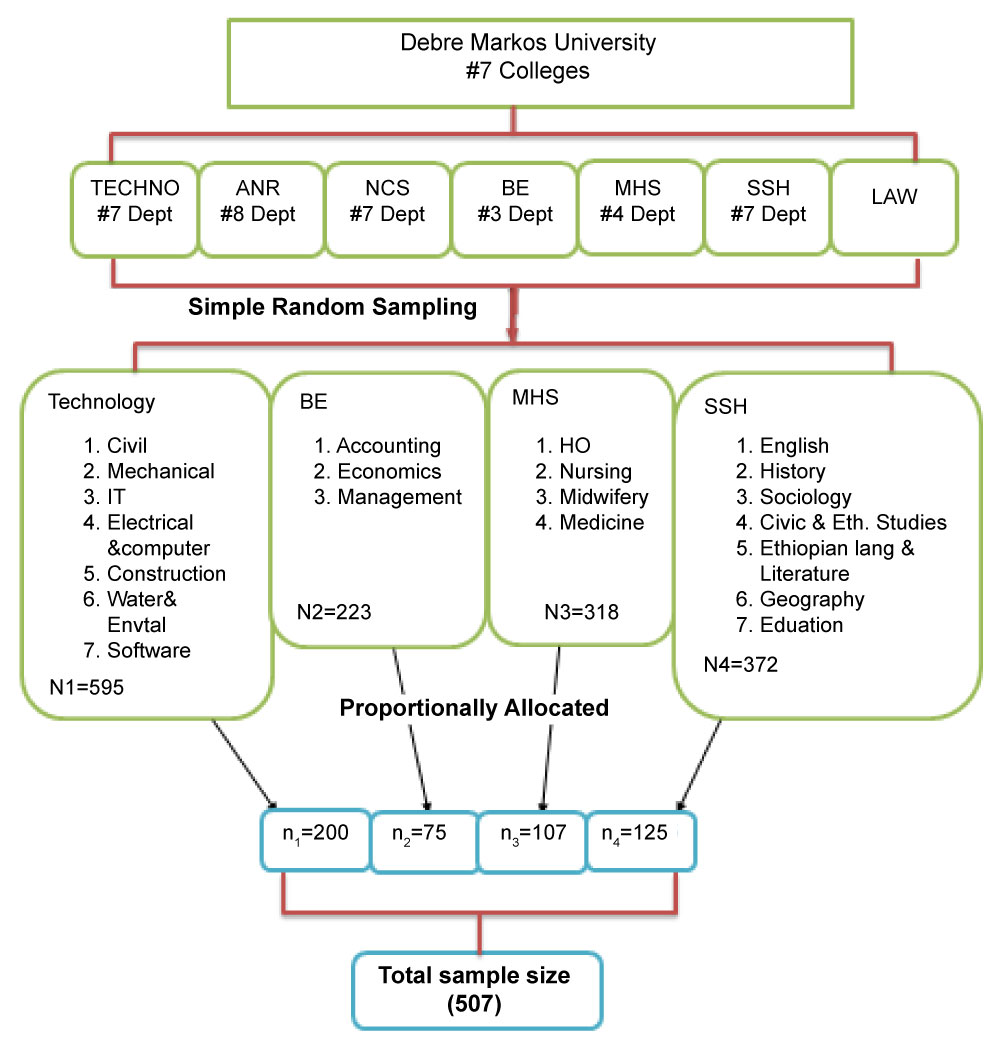 Figure 1: Schematic presentation of sampling procedure of female students in Debre Markos University, Northwest Ethiopia, 2016.
Figure 1: Schematic presentation of sampling procedure of female students in Debre Markos University, Northwest Ethiopia, 2016.
Hint: ANR: Agriculture & Natural resource; NCS: Natural & computational Science; BE: Business & Economics; MHS: Medical & Health Science; SSH: Social Science & Humanities; Ho: Health officers.
View Figure 1
Structured self-administered questionnaire prepared in English was translated to Amharic which is local language by language experts and translated back to English by other language experts to check its consistency. Amharic version questionnaire was used to collect data on socio-demographic, knowledge status of students towards Ethiopian liberal law of safe abortion, University educational status of student, reproductive health status variables, family status of the student and Source of information. Three diploma holder midwives with minimum two year work experience was selected randomly and one BSc midwifery holder was selected for supervision.
Pre-test was done on 26 (5% of sample size) on teacher training college (TTC) students found in Debre Markos town. Based on the finding grammatical sequences of questions were arranged on questionnaires. Training and orientation were given to the selected data collectors and supervisor for two days.
The Principal Investigator and Supervisor confirmed on the daily base the collected data for the completeness, accuracy and clarity with data collectors and necessary correction was made before the next data collection day started. Finally, data cleaning; data entry, coding and crosschecking was done before data analysis.
The collected questionnaires were checked manually for completeness. Then data was coded, labeled, verified, categorized and entered into Epi Info version 7. After the entry was completed the data was exported to SPSS version 20.0 for analysis. Descriptive and summary statistics was done. An Odds ratio (OR) with 95% confidence interval (CI) used to see the association between independent variables and a dependent (outcome) variable. Logistic regression analysis was used to determine the strength of association of each independent variable with the outcome variable. Variables significant in bi-variate analysis (P < 0.2) were entered into a multivariable logistic regression and checked with Hosmer-Lemeshow Goodness- of fit model to adjust the effects of possible cofounders on the outcome variable.
This study approved by Institutional Research Ethics Review Committee (IRERC) of College of Medicine and Health Science, University of Gondar. Supportive official letters was written to Debre Markos University by department of Midwifery College of Medicine and Health Science, University of Gondar. Information containing about the purpose, method and anticipated benefit and risk of the study was attached to the first page of each questionnaire. Participants' names and ID numbers was not included in the questionnaire for the purpose of keeping their confidentiality.
Outcome variable of this study was knowledge status of female students learning in Debre Markos University on liberalized safe abortion of Ethiopia. To measure level of knowledge, the mean values of the respondents to the five criteria under which safe abortion is legally permitted was calculated and taken as a cut point value to decide whether female students have good or poor knowledge about liberalized safe abortion of Ethiopia. Thus, female students who scored below mean value considered as having poor knowledge and those with mean and above score were regarded as having good knowledge. Socio-demographic variables including participants' age, marital status, religion, family residence, year of study, department of study, contraceptive use, having boyfriends and previous sexual exposure were independent variables.
All distributed questionnaires (507) were filled and returned but 24 questionnaires found to be incomplete and rejected from the analysis, making response rate of 95.3%. The mean age of respondents was 21.55 years (SD = ± 2.12). Three hundred eighty two (79.1%) were aged between 20-24 years. The majority (82.6%) of the respondents were single. About half (47%) were Amhara by ethnicity and 62.1% were Orthodox Christians. About two hundreds thirty three (48.2%) respondents father were illiterate and around 279 (57.8%) of respondent's mother were also illiterate and 10.6% of respondent's father and 5% respondents mother educational level were college/university graduate. Two hundred sixty one (54%) respondents family were living in rural area. For about 74.9% of the respondents, their father and mother are alive and only 3.5% of them have lost both of their parents (Table 1).
Table 1: Socio-demographic characteristics of respondents (n = 483), Debre Markos University, Northwest Ethiopia, April, 2016. View Table 1
About 199 (41.2%) of the respondents have knowledge about liberalized law of safe abortion (Figure 2). Nearly 188 (38.9%) of the study participants responded that safe abortion is legally permitted for all pregnancy. 260 (53.8%) of the respondents answered that safe abortion is legally permitted if the pregnancy is from incest and 254 (52.6%) responded safe abortion is legally permitted if the pregnancy is from rape. Three hundred seventeen (65.6%) reported that safe abortion is legally permitted if the continuation of the pregnancy endangers the life of the mother or the life of the baby. About 316 (65.4%) had awareness that safe abortion is legally permitted if the fetus has an incurable and serious deformity.
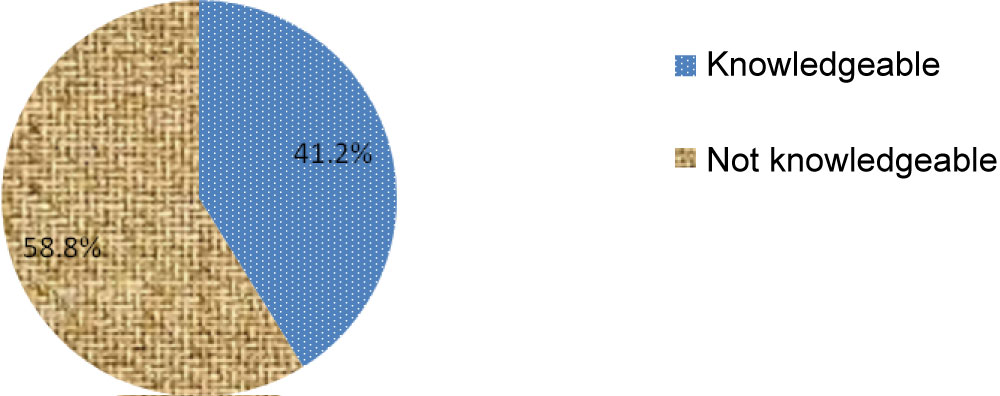 Figure 2: Knowledge level of Debre Markos University female students about criteria of safe abortion services, Northwest Ethiopia, April, 2016 (n = 483).
View Figure 2
Figure 2: Knowledge level of Debre Markos University female students about criteria of safe abortion services, Northwest Ethiopia, April, 2016 (n = 483).
View Figure 2
About a 311 (64.4%) of study participants responded that safe abortion is legally permitted if the pregnant woman was having physical problem or mental deficiency. Nearly half (47%) of respondents reported that Ethiopian liberal law of abortion permitted abortion up to 12 weeks gestational age and only 7.7% of them answered correctly as per Ethiopian liberalized safe abortion law which is up to 28 weeks gestational age. About two third of respondents reported both medical abortion and instrumental methods as method of abortion techniques and almost more than half of respondents had good awareness regarding complications of abortions (Table 2).
Table 2: Knowledge status of Debre Markos University female students about criteria safe abortion services, Northwest Ethiopia, April, 2016 (n = 483). View Table 2
About 187 (38.7%) of respondents had ever heard about liberalized safe abortion of Ethiopia. About thirty three percent of the respondents have got information on criteria under which abortion is legally permitted from teachers while only 6% reported mass media and others like their boyfriend and internet accounts for about 4.7%.
About 217 (44.9%) of the respondents in the study area had a boyfriend and 153 (31.7%) of the study participants responded that they had ever performed sexual intercourse. Among those who had sexual intercourse, 133 (86.9%) of them had sexual intercourse first in the age range of 15-20 years. And about 11.1% of them had sexual intercourse at 20 years and above.
About twenty one (53.85%) of respondent undergone abortion because of their education and one (2.6%) of them responded due to physical and mental problem (Figure 3). 39.8% of respondents were from technology faculty and 14.5% were from Business and Economics faculty. About 26.7% of respondents were first year and 20.7% of them were from fourth year and above (Figure 4 and Figure 5).
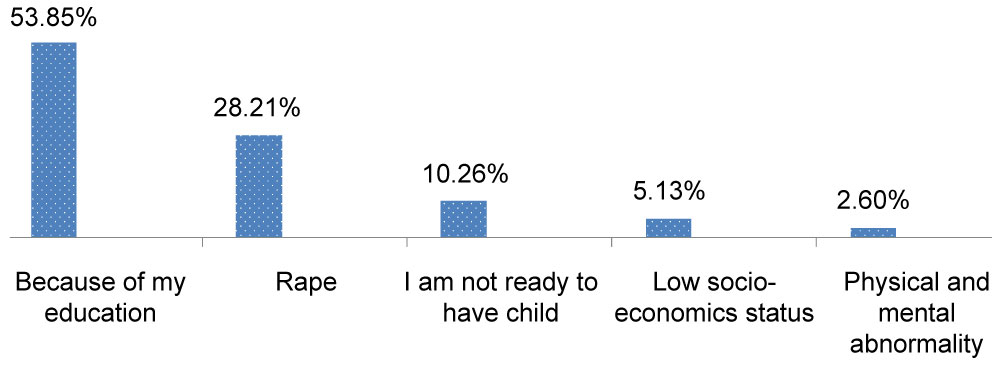 Figure 3: Distribution of respondent's reason of undergoing abortion in Debre Markos University female students, Northwest Ethiopia, April, 2016.
View Figure 3
Figure 3: Distribution of respondent's reason of undergoing abortion in Debre Markos University female students, Northwest Ethiopia, April, 2016.
View Figure 3
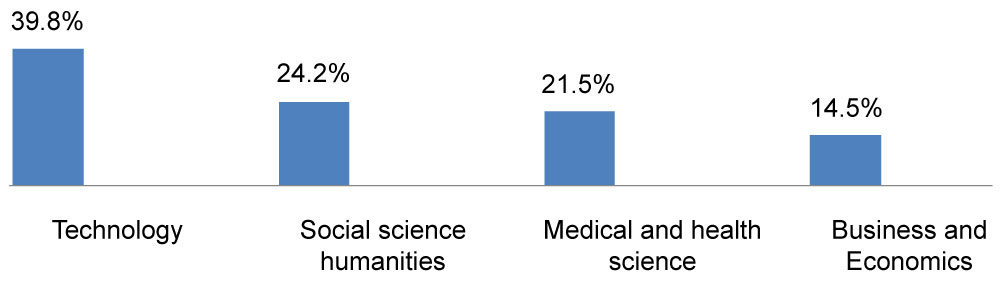 Figure 4: Distribution of respondent's field of study in Debre Markos University, Northwest Ethiopia, April, 2016.
View Figure 4
Figure 4: Distribution of respondent's field of study in Debre Markos University, Northwest Ethiopia, April, 2016.
View Figure 4
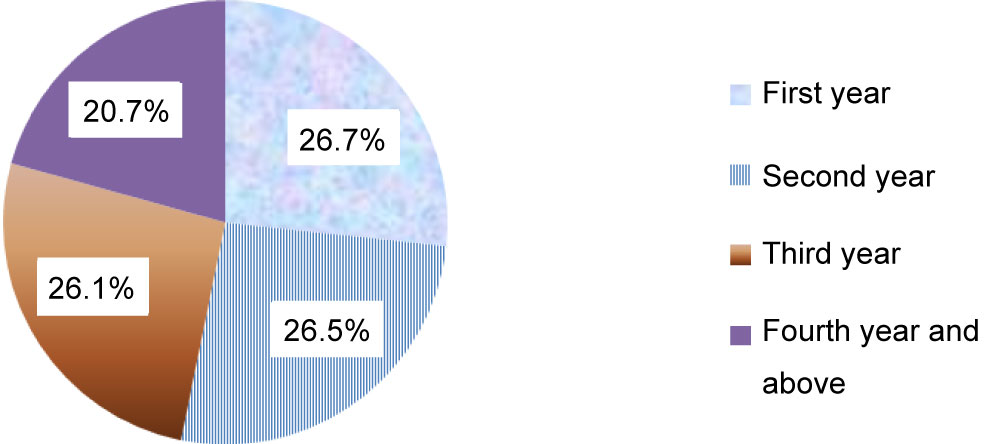 Figure 5: Distribution of respondent's year of study in Debre Markos University, Northwest Ethiopia, April, 2016.
View Figure 5
Figure 5: Distribution of respondent's year of study in Debre Markos University, Northwest Ethiopia, April, 2016.
View Figure 5
In bivariable analysis age, marital status, family residence, mother's educational status, having boyfriend/husband, ever become pregnant before, having sexual intercourse practice and field of study of respondents were significantly associated with knowledge of female students to liberalized safe abortion of Ethiopia (p-value < 0.2).
Multivariable logistic regression analysis showed that marital status, family residence, mother's educational level and ever had pregnant before were the factors that were significantly associated with knowledge of female students to liberalized safe abortion after possible confounders were controlled.
The finding from multivariable analysis indicated that those single participants were 2.7 times more likely to have knowledge compared to those who were married [AOR = 2.7, 95% of CI: (1.52, 4.79)]. Those respondents whose families live in rural were about 1.6 times more likely to be knowledgeable than those whose families live from urban area [AOR = 1.56, 95% of CI: (1.03, 2.39)]. Female students whose mothers were illiterate were about 2.66 times more likely to have good knowledge than whose mother's educational level were college/university [AOR = 2.68, 95% of CI:( 1.08, 6.61)]. Those students who had no pregnancy history were 10.68 times more likely to have knowledge about liberalized safe abortion than those who had history of pregnancy [AOR = 10.68, 95% of CI: (4.52,25.22)] (Table 3).
Table 3: Bivariable and Multivariable analysis of factors associated with knowledge of safe abortion among female students in Debre Markos University, Northwest Ethiopia, April, 2016. View Table 3
Even though Ethiopian liberalized safe abortion were amended in 2005, in this study only 41.2% of respondents were knowledgeable about safe abortion after eleven years. This finding is consistent with that study done in Nepal in which about 41% of respondents had good awareness about legalization of abortion law in their country [16]. Study in South Africa revealed that about 68% of study participants were knowledgeable about legal abortion law of their country [17], which is higher than current study and this difference may be due to socio-economic difference, their reproductive health service coverage, difference in quality of implementation of health interventions strategy and the time difference at which abortion is allowed in these countries. The similar study in Harari regional state in Ethiopia revealed only 35.7% of study participants had good awareness about liberal law of safe abortion [12] and from study done in Arba Minch higher education female students, only 32.1% had good knowledge about this issue which is less than the result of this study [15], this may be due to socio-cultural and time difference.
This study revealed that being single was more likely to have knowledge than those who were married which is opposite with study done in Gurage zone, South Ethiopia [18], this may be due to difference in study subjects which means in this study most of the students were single and prone to different health related information like mini media and youth associations. The finding of this study also showed that those females whose mother's were illiterate were more likely to be knowledgeable than those whose mothers attended college/university, which is in contrast to study done in Kenya and Gurage zone, South Ethiopia [18,19], this might be due to social desirability bias or may be the educated people may ignore to teach their daughters about safe abortion.
In addition this study revealed females whose families live in rural were more likely to be knowledgeable than those whose families live in urban. This finding is opposite with findings from Amhara region referral hospitals in which place of residence affects the respondent's knowledge about safe abortion [20]. This may be due to difference in study subjects. Those students who had previous pregnancy history were less likely to be knowledgeable than those who were not ever pregnant, this finding is reverse with the findings from female youths in Uganda [21].
Using the cross-sectional design was the limitation of the study. The social desirability bias due to the nature of the sensitivity issues of abortion and the past history on abortion might be affected by recall bias.
This study disclosed that there was high proportion of female university students with poor knowledge of liberal law of safe abortion in Ethiopia. Marital status of respondents, family residence, maternal education level and prior pregnancy experience were factors significantly associated with knowledge of female students towards liberalized safe abortion. Concerned bodies should be done on awareness creation about legal issues of safe abortion. Further research should be conducted to assess the knowledge of rural and less educated adolescents on liberal law of safe abortion.
The authors of this study confirmed that we have no any kind of conflict of interest.
• Biru Abdissa had contributions from beginning of the research idea to proposal writing, data collection process, data analysis and interpretation of finding and preparation of the manuscript.
• Abayneh Aklilu has contributed in proposal writing, analysis of the finding and preparation of the manuscript.
• Endeshaw Admasu has contributed in proposal development, analysis of finding, and interpretation of research finding.
• Sagni Girma has contributed in proposal writing, analysis of the finding and preparation of the manuscript.
✓ Biru Abdissa has Master of Science in Clinical Midwifery and currently working in Institute of Health Science, School of Nursing and Midwifery, Department of Midwifery, Jimma University as a lecturer.
✓ Abayneh Aklilu has Master of Science in Clinical Midwifery and currently working in College of Medicine and Health Sciences, Department of Midwifery, University of Gondar as a lecturer.
✓ Endeshaw Admasu has Master of Public health in Reproductive Health and currently working in College of Medicine and Health Sciences, Department of Midwifery, University of Gondar as an Assistant Professor.
✓ Sagni Girma has Master of Public health in Nutrition and currently working in College of Health and Medical Sciences, School of Nursing and Midwifery, Department of Nursing, Haramaya University as lecturer.
We would like to express our heartfelt thanks to University of Gondar, Midwifery department for the financial support to complete this research. We will also extend our thanks to Debre Markos University for their supportive cooperation and willingness in our process to do our research and finally, we thanks our data collectors and study participants.