The role of laparoscopy in abdominal trauma has increased in the last years in diagnosis as well as therapeutic interventions. It is a viable alternative for the diagnosis of intra-abdominal injury in both penetrating and blunt trauma. The number of negative laparotomies decreased since the use of laparoscopy in trauma patients.
A retrospective study of twenty eight patients with abdominal trauma (22 penetrating trauma, 6 blunt trauma) were laparoscopic intervention done by general surgery department at Aljazeera Hospital for Orthopedic and Specialized Surgery from January 2017 to March 2019. All patients underwent clinical assessment and FAST-Scan, CT-scan done for twenty patients and unavailable for eight patients. All of the patients included for the research were stable with normal blood pressure.
In our series twenty-eight patients with abdominal trauma, 22 penetrating trauma (78.57%) all were shotgun injuries, and 6 blunt trauma (21.43%). In penetrating trauma therapeutic laparoscopy for seven patients (31.8%), diagnostic laparoscopy for 10 patients (45.5%), and negative laparoscopy for 5 cases (22.7%). In blunt trauma therapeutic laparoscopy for 2 cases (33.3%), diagnostic laparoscopy for 3 cases (50%), and negative laparoscopy for 1 case (16.7%). The rate of conversion to laparotomies was 8 cases (28.5%) for both penetrating and blunt trauma.
Laparoscopy can be safely performed in hemodynamically stable patients with abdominal trauma for both diagnostic and therapeutic purposes; also it helps to cut down the number of non-therapeutic laparotomies.
Laparoscopy, Penetrating abdominal trauma, Blunt abdominal trauma
Explorative laparotomy is the traditional mainstay of management in patients with penetrating and blunt abdominal trauma [1]. In the 1960s, Shaftan first challenged the idea of mandated laparotomies for abdominal trauma with his term of selective conservatism, as half of his patients with penetrating abdominal trauma did not require operative repair [2]. In recent review, surgical exploration in the setting of penetrating abdominal trauma has been associated with negative laparotomy rates of about 61% [3]. Negative or non-therapeutic laparotomies are associated with 20% morbidity rate [4]. A reliable and consistent tool for identification of those patients with visceral and diaphragmatic injuries is by direct visualization either by diagnostic laparoscopy or laparotomy [5]. The advantage of laparoscopy can provide both diagnostic and therapeutic interventions for those hemodynamically stable abdominal trauma patients [6]. The solid organ and visceral injuries can be reliably assessed by laparoscopy, identification of intestinal injury is more challenging, however hollow organ injuries may display neither clinical signs of acute abdomen nor positive radiological signs in the early post-traumatic phase, subsequently delayed exploration with a higher risk of septic shock and increase morbidity ensue [7]. Laparoscopy can detect sign of visceral injury and repair it or convert to laparotomy [8]. Diagnostic laparoscopy must identify all injuries as effective as computed tomography. There is a large range in the number of abdominal injuries that can be treated laparoscopically in trauma setting [9]. The subset of patients presenting with penetrating trauma combined with vital stability and no clinical abdominal signs warrants more complex decision making [10]. It is in this subset where laparoscopy constitutes a useful tool potentially eliminating of non-therapeutic laparotomies and conservative management, namely delay exploration which need prolonged hospital stay and costs associated with serial labs and imaging [11].
To determine the safety and efficacy of laparoscopy in hemodynamically stable abdominal trauma patients.
A retrospective study of twenty eight patients with abdominal trauma (22 penetrating trauma, 6 blunt trauma) were laparoscopic intervention done by general surgery department at Aljazeera Hospital for Orthopedic and Specialized Surgery from January 2017 to March 2019. All patients underwent clinical assessment inform of history and full body examination and Focused Assessment with Sonography for Trauma (FAST) Scan, Computed Tomography (CT) scan done for twenty patients and was unavailable for eight patients. All of the patients included for the research were stable with normal blood pressure. In patients with blunt abdominal trauma were an unexplained free fluid seen in imaging study or showing deterioration in clinical signs as fever, abdominal tenderness, and decrease hemoglobin levels are typically evaluated by a laparoscopic exploration. In patients with penetrating abdominal trauma and hemodynamically stable are evaluated by laparoscopic exploration. Operative interventions with laparoscopy were classified as therapeutic which includes hemostasis, repair or resection of any injured structure including solid organ or hollow viscus, and diaphragmatic repair. Diagnostic laparoscopy is a term used for abdominal injuries not requiring hemostasis or repair as in retroperitoneal hematoma. Negative laparoscopy is a term used in a case were abdominal organ injury not identified. Laparoscopic exploration is performed with a patient in supine position. Pneumo-peritoneum created by veress needle technique. First trocar usually at supra-umbilical area 10 mm trocar. The other trocars inserted according to the finding in the intra-abdominal cavity. All abdomen explored systematically including solid organs, hollow viscus and diaphragm.
In our series twenty-eight patients with abdominal trauma, 22 penetrating trauma (78.57%) all of them were shotgun injuries, and 6 blunt trauma (21.43%). In penetrating trauma therapeutic laparoscopy for seven patients (31.8%), diagnostic laparoscopy for 10 patients (45.5%), and negative laparoscopy for 5 cases (22.7%). Therapeutic laparoscopy were done for the following cases, two cases liver tears were hemostasis done by combined of cauterization and intra-corporeal stitching, three cases of diaphragmatic injury were repaired by intra-corporeal stitching, one cases of splenic tear were bleeding not stopped with cauterization and splenectomy done, last case was small bowel perforation were repaired with intra-corporeal stitching. Diagnostic laparoscopy were done for the following cases, seven cases were injuries diagnosed and converted to laparotomies including three major liver injuries, splenic injury with active bleeding, huge diaphragmatic injury, and two combined large and small bowel injuries, while the last two cases of diagnostic laparoscopy not converted were retroperitoneal hematoma identified. In blunt trauma therapeutic laparoscopy for 2 cases (33.3%), diagnostic laparoscopy for 3 cases (50%), and negative laparoscopy for 1 case (16.7%). Therapeutic laparoscopy were done for the following cases, one case of diaphragmatic injury and repaired by laparoscopy, and one case of grade 4 splenic injury were laparoscopic splenectomy done. Diagnostic laparoscopy were done for the following cases, one case of large diaphragmatic injury were converted to laparotomy, two cases of retroperitoneal hematoma. The rate of conversion to laparotomies were 8 cases (28.5%) for both penetrating and blunt trauma. No complications were associated with pneumoperitoneum (Figure 1, Figure 2 and Table 1).
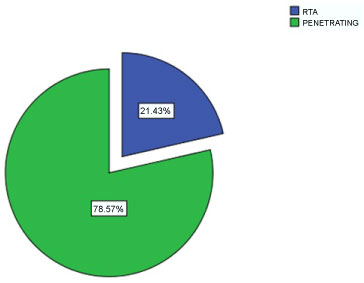 Figure 1: Type of injury. View Figure 1
Figure 1: Type of injury. View Figure 1
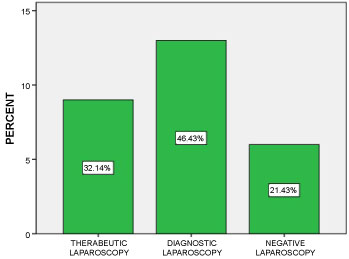 Figure 2: Classification of laparoscopic procedures. View Figure 2
Figure 2: Classification of laparoscopic procedures. View Figure 2
Table 1: Laparoscopy finding and procedure. View Table 1
The application of laparoscopy increasing with technical advances and increasing experience with its use in management of acute surgery including trauma surgery [12,13]. In the earliest work of laparoscopy in trauma, Gazzangia, et al. evaluated 37 patients, they found 14 of these patients laparotomy was avoided because of a negative diagnostic laparoscopy [14]. There were no false negative investigations, they concluded that the use of diagnostic laparoscopy in abdominal trauma had advantages to decrease the rate of negative laparotomy [14]. In the largest study performed on role of laparoscopy in penetrating abdominal trauma, Ivatury's group [15] reported a multicenter retrospective study of 510 hemodynamically stable patients underwent diagnostic laparoscopy for penetrating trauma, negative or non-therapeutic laparotomy was avoided in 303 (59.4%) patients, and 26 patients received a therapeutic laparoscopic intervention [15]. Chol and Lim performed a laparoscopy for 78 stable patient who already underwent CT scan revealed a significant injuries, two third of his patients were blunt trauma, this group reported no missed injuries, no mortality with (83%) success rate to complete it by laparoscopy [9]. While data from other institutions show higher rates of complications and missed injuries and narrower range of therapeutic intervention by laparoscopy [5,16].
In our series twenty-eight patients with abdominal trauma, 22 penetrating trauma (78.57%), and 6 blunt trauma (21.43%). In penetrating trauma therapeutic laparoscopy for seven patients (31.8%) were (13%) in [7], diagnostic laparoscopy for 10 patients (45.5%) were (33%) in [7], and negative laparoscopy for 5 cases (22.7%) but was (11.5%) in [17]. Therapeutic laparoscopy were done for the following cases, two cases liver tears were hemostasis done by combined of cauterization and intra-corporeal stitching, three cases of diaphragmatic injury were repaired by intra-corporeal stitching, one cases of splenic tear were bleeding not stopped with cauterization and splenectomy done, last case was small bowel perforation were repaired with intra-corporeal stitching. The most common penetrating abdominal injury was liver injury and was the same in [18].
Minimal invasive surgery become a useful tool in the treatment of the abdominal trauma, laparoscopy can diagnose and repair injuries to hollow viscus, diaphragm and solid organs [12]. Further advantages are reduced morbidity, shortened hospital stay and lower cost [12].
Laparoscopy can be safely performed in hemodynamically stable patients with abdominal trauma for both diagnostic and therapeutic purposes; also it helps to cut down the number of non-therapeutic laparotomies.