The aim of the study is to validate two high-incline Graded Exercise Tests (GXT) that could be used as alternatives to the Bruce protocol to obtain VO2max values for college-aged individuals who may not be accustomed to running on a treadmill.
Subjects (n = 42, male = 25, female = 17, age = 23.2 ± 2.6 years) completed the Bruce protocol as well as two high-incline GXTs (5-5, 10-5) in a randomized order. Both high incline VO2max tests were performed at a constant speed of 3.6 mph and increased in incline of 5% every 3-minutes until volitional exhaustion. The 5-5 began with a 5% grade, while the 10-5 began with a 10% grade. Outcome measurements of VO2max were compared using a 1 x 3 repeated measures ANOVA. Pearson Correlation and Bland-Altman plots were used to analyze relationships between the two high-incline tests and the Bruce protocol individually.
No differences in VO2max was found between tests (Bruce = 45.99 ± 7.57 ml∙kg-1∙min-1, 5-5 = 44.97 ± 7.71 ml∙kg-1∙min-1, 10-5 = 43.99 ± 8.01 ml∙kg-1∙min-1, p > 0.05). VO2max of the Bruce protocol was strongly related to both 5-5 (R = 0.95) and 10-5 (R = 0.91) tests. Bland-Altman plots between the 5-5 test and the Bruce protocol revealed 93% of data falls within ± 4.5 ml∙kg-1∙min-1 of the arbitrary accepted range. For comparison between 10-5 and Bruce, variability increased as only 79% of the data fell within the same arbitrary range.
Results suggest that the 5-5 test is a valid alternative to the Bruce protocol. Additionally, the current study demonstrates that a non-running GXT is effective in determining VO2max in a relatively healthy, college-aged population.
VO2max test, Bruce protocol, Non-running, Injury prevention
Maximal oxygen uptake (VO2max) assesses the upper limit of an individual's ability to consume and utilize oxygen during intense, or maximal exercise, commonly accepted as a reliable indicator of cardiorespiratory health [1,2]. It is also an important marker for chronic conditions as reduction in VO2max has found to associate with obesity, type 2 diabetes, and heart failures [3]. As such, measurements of VO2max provide valuable diagnostic information for the design and evaluation of long-term exercise intervention in both research and clinical settings [4]. Numerous attempts have been made in past decades to develop accurate testing models of VO2max for different populations including children, older adults, and secondary individuals [5-7]. These models differ in duration, mode, and work rates, aiming for certain levels of cardiac response that could be used to predict VO2max.
Among all the existing protocols, Graded Exercise Tests (GXT) that require direct measures of oxygen uptake through continuous gas analysis are preferred when possible [2]. The Bruce maximal treadmill test developed in 1973 is one of the most commonly practiced GXT for assessing VO2max in both athletic and clinical settings [2,8]. The Bruce protocol has proven to be time efficient and suitable across a broad range of age groups [4,9,10]. However, some individuals may have difficulty completing the Bruce protocol consequent to the required transition from walking to running in the later stages of the test, which might be challenging for people who are less fit or unfamiliar with treadmill exercise. As suggested by the American College of Sport Medicine (ACSM), selection of VO2max tests should consider individual characteristics such as age, gender, and fitness level since they are all important factors that influence oxygen consumption during exercises [2]. Therefore, an alternative walking only VO2max protocol appears to be more suitable for those unaccustomed to treadmill running.
One population that could benefit from a VO2max test protocol that does not involve running are millennial college aged students. In today's society, technology advancement has transformed all aspects of the millennial life style with nearly every college student owning at least one small mobile device [11,12]. However, the increased access and usage of technology have been associated with growing rates of obesity and prevalence of physical inactivity in colleges [12-14]. Irwin reported that more than half of the college students in the United States and Canada failed to meet the ACSM recommendations for physical activity [15]. Other studies on international areas have found similar percentages of college students who were not physically active (20%-80.6%) [16-19]. These findings suggest that many college students, due to their secondary behaviors, might be unfamiliar with exercise equipment including treadmills and potentially have difficulties performing maximal GXTs such as the Bruce protocol at running speeds.
Therefore, to provide a more participant-friendly testing model for college-aged individuals who are less experienced with running on a treadmill, two walking only protocols were created using incline as workload increase while speed remined constant. These two proposed VO2max protocols are compared to the Bruce protocol for validation in the present study.
A total of 42 subjects (25 male, 17 female, age 23.2 ± 2.6 y, height 69.2 ± 4.2 in, weight 167.6 ± 39 lbs), with varying fitness levels were recruited. All subjects completed a pre-exercise questionnaire (PARQ+) to identify any potential health risks. Institutional Review Board at Brigham Young University-Idaho approved the project, and all subject gave their informed consent prior to the start of the study.
The new 5-5 and 10-5 protocols that have been developed maintain a constant speed at 3.6 mph while incline increased steadily. Speed was set based on that most people struggled (possibly maxed out) at 2 mph with 40% incline. This equated to about 3.3 W/kg (watts = power per mass for any given individual). Watts were calculated from the force (weight of the individual). From this data, a mathematical optimization was performed to find the speed at which someone would need to walk to achieve up to 4 W/kg in five stages. From that optimization, it was discovered that 3.6 mph would achieve 3.88 W/kg at 25% incline, which is just under 300 watts for someone who weighs 75 kg. Therefore, except for the very fit, this would tax the system within the correct amount of time for a VO2max test. This equation is applicable for sedentary individuals or individuals that struggle to maintain a running pace for extended periods of time [unpublished study]. A true VO2max is achieved by a limited change in VO2 despite an increase in workload. Incline served as the increase in workload because speed remained constant.
Subjects were asked to fast for a period of 3 hours and refrain from vigorous exercises for 24 hours prior to testing. The three GXTs completed by each subject included the Bruce protocol, the 5-5 protocol, and the 10-5 protocol. VO2max tests were completed until volitional exhaustion in a randomized cross-over order by each subject. After performing all three tests, subjects were asked to identify which GXT they preferred the most. A two-day recovery period was given between tests.
All tests were performed on NordicTrack X9i and X11i (ICON, Logan, UT) treadmills. Treadmill incline calibration occurred following the completion of three tests. Speed of the treadmill was also calculated for each stage of the Bruce protocol for accuracy, as well as for the first stage of 5-5 protocol and 10-5 protocol. Each subject was fitted with an oxygen consumption mask (Hans Rudolph, Shawnee, KS) to collect expired gases throughout testing. Metabolic data and expired gases were taken breath by breath and averaged for every 15 seconds using a computerized metabolic system (Parvo Medics Trueone 2400, Murray, UT). Heart Rate (HR) was continuously recorded using Polar Heart Rate Monitors (Polar, Bethpage, NY). Rate of Perceived Exertion (RPE) using the Borg's 15-point scale was collected during the last 15 seconds before each stage ended [20]. During each test, words of encouragement were given to help coach subjects to maximal exertion, after which subjects performed a walking cool down period at self-selected pace, incline, and time.
The Bruce protocol consists of starting at 1.7 mph at 10% grade. Workload for both speed and incline increased subsequently every 3 minutes according to Table 1. The 5-5 protocol consists of 3-minute stages. Subjects started with a 30 seconds warm-up at 3.6 mph with no incline, thereafter, stage one began at 5% immediately and incline increased by 5% each 3-minute period. The 10-5 protocol was identical to the 5-5 with the only difference of having the starting grade set at 10%. Treadmill speed maintained at 3.6 mph for both 5-5 and 10-5 tests. The tests were terminated when subjects were unable to maintain the required pace or reached volitional exhaustion. After each test all subjects were asked to report a reason for termination.
Table 1: Comparison of stage workload between three protocols. View Table 1
A subject's final VO2max was determined as the highest oxygen uptake measured during the last minute of each test. VO2max values were considered acceptable if they met at least three of the four commonly accepted criterion: (1) RPEmax value ≥ 17 [21]. (2) Heart rate (HR) within 15 beats of age-predicted maximum heart rate (208 - (age*0.7)) [22]. (3) Respiratory exchange ratio (RER) value ≥ 1.10 [23]. (4) Plateau of oxygen uptake despite an increase in workload (< 2.0 ml*kg-1*min-1 increase) at least 1 minute into the last stage [24].
Outcome measurements of VO2max for all three maximal exercise protocols were compared using a 1 × 3 repeated measures ANOVA. VO2max values from the 5-5 and 10-5 protocols were compared separately to the Bruce protocol. A Pearson Correlation analysis was performed for each comparison to obtain an R value. Bland-Altman analysis was performed to assess agreement between each of the proposed protocols and the Bruce protocol. Interpretation of Bland-Altman used a prespecified range of ± 4.5 ml*kg-1*min-1 to represent acceptable VO2max variance between tests [9,25]. A one-sample T test was used to determine if treadmill speeds were significantly different throughout the duration of the hypothesized protocols. Statistical significance was set at p < 0.05.
Performance data for all protocols are presented in Table 2. For the Bruce protocol all subjects reached the criteria for VO2max. For the 5-5 protocol 41/42 reached the criterion for VO2max. For the 10-5 protocol 39/42 reached the criterion for VO2max. Repeated measures ANOVA showed no differences in VO2max between tests (Bruce = 45.99 ± 7.57 ml*kg-1*min-1, 5-5 = 44.97 ± 7.71 ml*kg-1*min-1, 10-5 = 43.99 ± 8.01 ml*kg-1*min-1, p > 0.05).
Table 2: Comparison of performance variables between groups (average ± standard deviation). View Table 2
The 5-5 protocol was found to be highly correlated to the Bruce protocol with an R value of 0.95 (Figure 1); whereas the correlation between the 10-5 and the Bruce was relatively lower (R = 0.91, Figure 2). Interpreting the Bland-Altman comparison for the 5-5 to Bruce protocol showed that 100% of VO2max data falls within a range of -4.7 to 4.8 ml*kg-1*min-1, and 93% of the value falls within the arbitrary accepted range of ± 4.5 ml*kg-1*min-1 (Figure 3). For the comparison between 10-5 and the Bruce protocol, variability increased as only 79% of the data falls within the accepted range of ± 4.5 ml*kg-1*min-1. (Figure 4).
 Figure 1: Scatter plot of measured VO2max with correlation trendline and R value between the 5-5 and the Bruce protocol.
View Figure 1
Figure 1: Scatter plot of measured VO2max with correlation trendline and R value between the 5-5 and the Bruce protocol.
View Figure 1
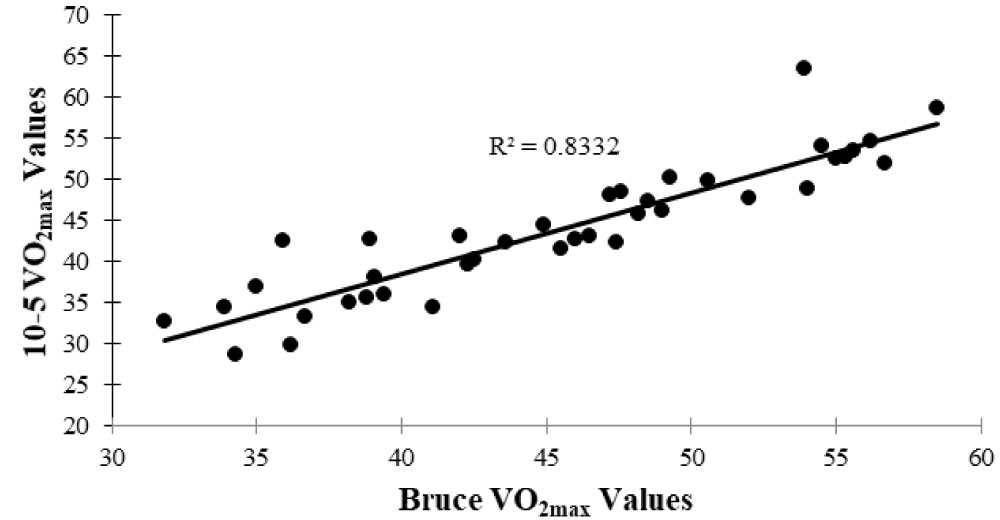 Figure 2: Scatter plot of measured VO2max with correlation trendline and R value between the 10-5 and the Bruce protocol.
View Figure 2
Figure 2: Scatter plot of measured VO2max with correlation trendline and R value between the 10-5 and the Bruce protocol.
View Figure 2
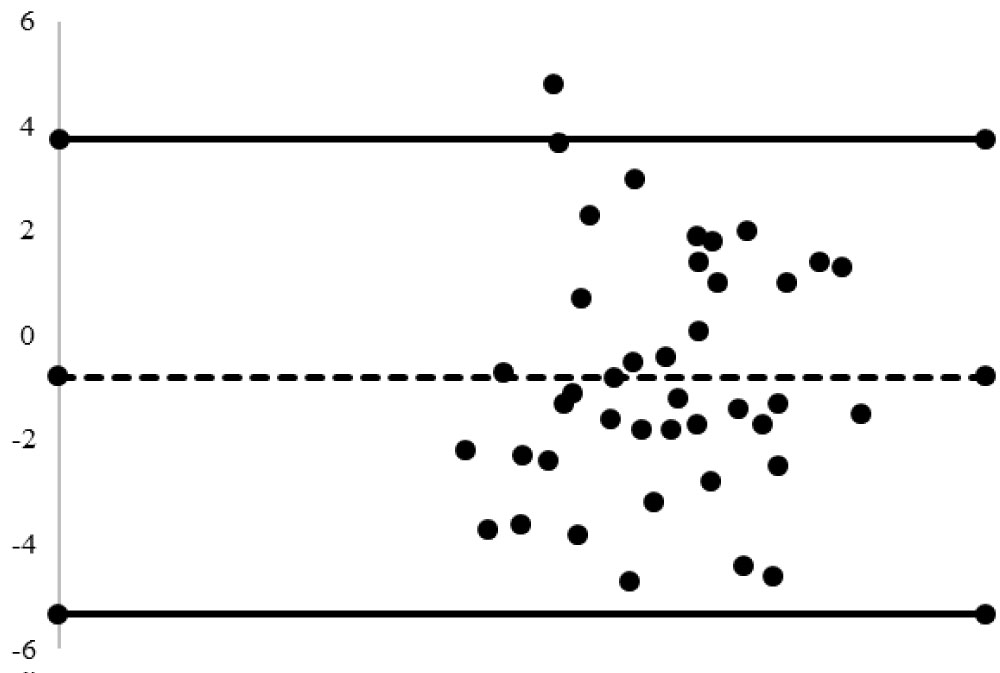 Figure 3: Bland-Altman analysis of the 5-5 and the Bruce protocol. Solid lines represent the upper and lower limits of agreement. Dotted line represents the average difference the 5-5 protocol had from the Bruce protocol. 93% values within acceptable range of ± 4.5 ml*kg-1*min-1.
View Figure 3
Figure 3: Bland-Altman analysis of the 5-5 and the Bruce protocol. Solid lines represent the upper and lower limits of agreement. Dotted line represents the average difference the 5-5 protocol had from the Bruce protocol. 93% values within acceptable range of ± 4.5 ml*kg-1*min-1.
View Figure 3
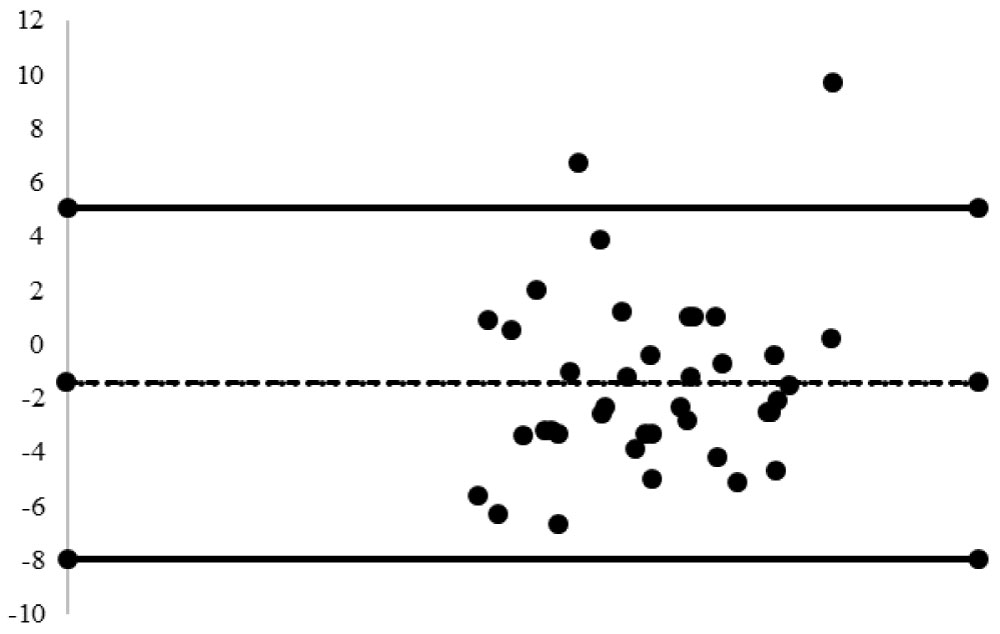 Figure 4: Bland-Altman analysis of the 10-5 and the Bruce protocol. Solid lines represent the upper and lower limits of agreement. Dotted line represents the average difference the 10-5 protocol had from the Bruce protocol. 79% values within acceptable range of ± 4.5 ml*kg-1*min-1.
View Figure 4
Figure 4: Bland-Altman analysis of the 10-5 and the Bruce protocol. Solid lines represent the upper and lower limits of agreement. Dotted line represents the average difference the 10-5 protocol had from the Bruce protocol. 79% values within acceptable range of ± 4.5 ml*kg-1*min-1.
View Figure 4
One sample T-Tests for the proposed alternative protocols demonstrated that treadmill speed was not statistically different between individual tests (P > 0.05). Half (21/42) of the subjects preferred the 5-5 protocol, 36% (15/42) preferred the Bruce protocol, and 14% (6/42) preferred the 10-5 protocol.
The current study was performed on subjects mainly from the millennial generation, with an average age of 23-years-old. The millennial generation is a renowned sedentary generation with a heavy reliance on technology which has been linked to a proliferating obesity rate. Kautiainen, et al. performed a study that showed a positive association between the increased use of technology and number of adolescents being overweight in Finland [26]. It is imperative to understand nevertheless, that the range of the obesity epidemic has spread throughout the entire globe and is no longer confined to high or middle-income countries [26,27]. This is partially because technological advances have caused the human race to deviate immensely from the normal activities of their ancestors [28]. Transportation by vehicle as opposed to by foot, and supermarkets that eliminate the need to hunt and gather are great examples of how technology has led to a decline in physical activity. Therefore, some millennial individuals may not be accustomed to running daily, and perhaps even less familiar with running on a treadmill, subsequently result in a decrease in the ability to perform maximal graded exercise tests at running speeds. Therefore, the 5-5 and 10-5 protocol were created to be better alternatives to the Bruce protocol for sedentary but healthy individuals of the millennial generation, because the methodology of the 5-5 and 10-5 protocol only requires subjects to walk. Additionally, the constant speed maintained throughout both proposed protocols allows for less adjustments and may make the subject feel more comfortable. Contrarily, the Bruce protocol starts with subjects walking slowly on a treadmill with increased speeds every three minutes, then after about nine minutes, subjects are set at a running pace with a high incline which may be problematic for sedentary individuals since many are unpracticed in running and maybe even be new to running on a treadmill.
Another concern with using the Bruce for testing unpracticed runners is that if not given sufficient time to become familiar with running on the treadmill, supplemental to a higher risk of injury, the data collected might be inaccurate as a result of inexperience. While the exact time it takes novice runners to become familiar with running on treadmill is relatively unstudied, it is understood that a familiarity phase does take place in getting accustomed to running on a treadmill, even in experienced runners [29]. One study conducted on college distance runners with significant over-ground running experience concluded that a familiarity phase of 8 minutes was needed for acclimation to running on a treadmill [29]. Acclimation in amateurish runners may very well take longer but needs further investigation. On the other hand, Lavcanska, et al. and Taylor, et al. set out to determine how long it takes for subjects unaccustomed to walking on a treadmill to become familiarized [30,31]. Lavcanska, et al. found no significant differences in the angles of the pelvis, hip joint, knee joint, and ankle joint after 6 minutes of walking on a treadmill compared to ground walking [30]. This is similar to the findings of Taylor, et al. that angular movements of the lumbar spine and pelvis could be reliably measured after 4 minutes of treadmill walking [31]. These findings are reinforced by the research of Matsas, et al. [32]. For this reason, it could prove problematic using the Bruce protocol since VO2max values of the Bruce was obtained on average 3-minute following the walk to run transition stage which occurs at the nine-minute mark. Three minutes was not considered adequate time to become accustomed to walking horizontally on a treadmill, let alone running on a treadmill at increasing inclines [30-32]. With VO2max being reached on average with only three minutes of treadmill running the Bruce protocol may not be the best suited test for a sedentary population not accustomed to running.
Walking has proven to be a good exercise alternative to running when individuals are not well conditioned to run or when running would further exacerbate existing lower extremity injuries [2]. In a previous study, Õunpuu found that running requires an increase in joint range of motion, forces, muscle activation, joint moments, and joint powers in comparison with walking [33]. Mann and Hagy also investigated biomechanical differences in walking, jogging, and running [34]. Results concluded that there is increased flexion of the hips, knees, and an increase in dorsiflexion at the ankle joint. Not only is there an increase in flexion, but also an increased speed of flexion in these joints. Mann and Haggy also found the hip joint to be a particularly crucial component of running, suggesting that walking would be more suitable for subjects with hip joint injuries [34]. Based on these findings, the 5-5 protocol may be a more appropriate protocol to test the VO2max of subjects with contraindications to running.
There have furthermore been positive findings associated with lower impact on joints when walking at inclines ranging from above horizontal to approximately 20% incline [35,36]. On average, subjects terminated the 5-5 protocol at approximately 20% incline, which could prove beneficial to subjects desiring a lower impact GXT protocol. Haggerty, et al. performed a study that tested walking on a treadmill at different grades ranging from 0% to 20% [35]. Results showed that peak internal knee-abduction moment decreased when walking at grades higher than 5%. This decrease may have positive effects on knee joint health and decrease the risk of injury. Moreover, at higher inclines knees are more flexed on impact which reduces the blunt force on the knee and significantly reduces risk for injury [35]. Another region of discomfort could be the plantar region. Ho, et al. found that peak pressures were significantly decreased with an increase of slope at the heel, medial forefoot, toe, and hallux [36]. The overall peak pressure of the plantar region decreased by 27% from 0% to 15% grade. Ho, et al. also found that the first striking position of the foot changes with incline from the heel to the midfoot, but ankle motion is not changed [36]. These findings reinforce the resultant increases of incline in the 5-5 protocol and infer the 5-5 protocol could be desirable for individuals with existing joint pain.
To assess the validity of other VO2max protocols proposed for the college population, results also included the correlation value between the Bruce protocol and the ASU protocol [9], which featured self-selected speeds. The ASU protocol aimed to provide a more individualized testing, but the protocol faced similar limitations to the Bruce protocol as a result of the running only speeds selected by subjects (4.1-6.7 mph). The ASU protocol was developed for the use of self-selected speeds, but because only running speeds were used to validate the protocol more research needs to be done to determine whether it is an effective GXT protocol that can include walking speeds in addition to running speeds. To our knowledge, there are three other protocols that instruct subjects to walk at high inclines with a predetermined speed for the entirety of the GXT: The 1959 Balke-Ware protocol [37], the 1977 USAFSAM protocol [38], and the "Slow" USAFSAM protocol [38]. The "Slow" USAFSAM protocol uses a slower constant speed and is mostly used on older patients and women. Wolthuis, et al. compared the USAFSAM protocol to the Balke-Ware protocol and showed a 24% reduction in time to exhaustion, suggesting the USAFSAM protocol is a more time effective GXT [38]. However, the validation of USAFSAM included mostly relatively fit subjects, and for this reason, the 5-5 and 10-5 walking only GXT protocols might be better suited to the sedentary millennial generation.
With the variety of available protocols, it is not only important to find those that can accurately measure aerobic capacity, but are also preferred by the specific individual. The hedonic theory applied in sport psychology states that individuals are more motivated to participate in exercises that bring pleasure or tailored to their physical abilities [39]. This is important in maximal graded exercise tests as motivation and enjoyment can largely affect whether the subjects push themselves to true exhaustion and subsequently yield accurate VO2max values. Therefore, a preference survey was conducted following the completion of all three GXT protocols to determine if subjects favored one protocol over the others. The survey concluded that more subjects preferred the 5-5 protocol over both the Bruce and 10-5 protocols (Table 2), suggesting that a walking only GXT protocol with a lower initial incline is valuable in terms of exercise prescription for the millennial generation as these young adults voted in favor of walking over running.
Evidence has also proven that the 5-5 is a valid method to attain a VO2max as compared to the accepted standards of the Bruce protocol through Bland-Altman plots. An accepted range difference of ± 4.5 ml kg-1 min-1 established by Fenstermaker, et al. was implemented for the comparison [25]. Results for the 5-5 protocol determined that 93% of the VO2max data fell within this accepted range, showing a strong similarity to the Bruce protocol. Variability increased for the 10-5 protocol as only 79% of the VO2max data fell within the accepted range. The 5-5 also has narrower lower and upper limits of agreements than the 10-5, proving the 5-5 protocol to be closer in accuracy to the Bruce and is an acceptable alternative GXT. Furthermore, Pearson Regression analysis showed a correlation coefficient (R-Value) of 0.95 between the VO2max data of the 5-5 and Bruce protocols, indicating a very strong correlation between the two. VO2max data from the 10-5 protocol had an R-value of 0.91 when plotted against the Bruce, showing less of a correlation than the 5-5 protocol. The 10-5 protocol also had the most subjects terminate the GXT before meeting required criteria for achieving VO2max, shorter average elapsed treadmill time to exhaustion, and lower overall VO2max values (Table 2). When asked the reason for their termination during the 10-5 protocol, most subjects reported leg fatigue as being the main factor. This was possibly due to the higher initial grade (10%) leading to a steeper climb than the 5-5 protocol.
In conclusion, the 5-5 protocol is a proven alternative to the Bruce protocol. The 5-5 protocol may be better suited for college-aged subjects with lower extremity injuries or are unfamiliar with running on a treadmill. Like the Bruce protocol, an accurate VO2max value can be obtained in a standardized and reproducible GXT within 12-15 minutes. It is reasonable to carry out future studies with the 5-5 protocol, using different populations and the same optimization technique to achieve specific speeds for each separate population. Information from this research can be used and expanded to further improve GXT protocols that elicit true fitness levels for special populations.
DEL was the primary investigator who oversaw the study; JB, LG, YW participated in data analysis, manuscript preparation, and manuscript editing; KH, LG, and TH carried out the study design, data collection, and data analysis. All authors have read and approved the final version of the manuscript and agree with order of presentation of the authors.
Dr. Lankford has performed research consulting for ICON Health & Fitness, manufacturer of the treadmills used in the study. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.