Information on the profile of dancers as well as patterns and extent of dance injuries is useful to dance community in implementing injury prevention measures. However, there is little published data on injuries in the Singapore dance population.
A prospective study was conducted to profile the dancers and study the incidence and injury patterns of a contemporary dance company.
Nine dancers underwent anthropometric measurement, dance specific screening as well as Functional Movement Screen (FMS). The dancers were interviewed for each injury that developed over a year to establish diagnosis as well as gather data on the circumstances surrounding each injury.
All the dancers were trained in multiple dance genres and had been dancing for a median of 10 years. Median age and body mass index were 27.4 years and 19.1 respectively. The dancers performed well in dance specific tests and were are largely symmetrical in posture and flexibility but had asymmetrical hip weaknesses. The dancers scored highly on the Functional Movement Screen (range 18-19) but had a wide range of aerobic fitness on the YMCA step test. A total of 15 injuries were reported and only one injury resulted in cessation of dance practice and for 1-2 days only. Of these, 46.7% had previous injuries in the same area, 53.3% were overuse injuries and 66.7% occurred during rehearsals. While not reaching statistical significance, a trend towards higher fatigue rating (median 6.5) with a median of 18 hours of training in the preceding week, was seen in injured dancers. Only 20% sought medical care and only 6.7% saw a physician.
The incidence of dance injuries was low. The dancers had asymmetrical weakness of the hip and lo aerobic fitness. Most injuries were mild and occurred through repetitive practice in novel movements during rehearsals. Fatigue may be a significant contributing factor to injuries especially during rehearsals. Injury prevention measures could be targeted at addressing fatigue through supplementary aerobic training and strength training.
Dance, Injury, Prevention, Surveillance, Prospective, Fatigue, Contemporary, Singapore
Dance training and performance subject the body to considerable physical stress. Physiological demands of dance, especially during performances, approximate that of sports with aesthetic elements such as gymnastics [1]. In addition, the training load increases during performance season which results in fatigue and increases the risk of musculoskeletal injuries [2].
Data such as anthropometric profiling, dance specific test results and competency in fundamental movement patterns of dancers and injury patterns guide injury prevention measures.
There is little research on dance injuries or practices in Singapore, with publications mainly limited to case studies or physiological studies [3,4]. A recent cross-sectional study on injury patterns in Singapore studied a heterogenous dance population which limited the inferences on causative factors that can be drawn from the study [5].
To conduct a prospective descriptive study on a semi-professional contemporary dance company and characterise the injuries that arise over one year.
To profile the dancers' physical characteristics through comprehensive screening which includes dance relevant anthropometric measurements, dance specific capabilities and the assessment of movement efficiency with Functional Movement Screen.
To explore the resources necessary to conduct dance specific screening and injury surveillance for a dance company over one year.
The study underwent ethics review by the National Healthcare Group Domain Specific Review Board. Upon approval, nine dancers from a contemporary dance company were recruited to participate in the study.
The screening was conducted for all dancers in a one-hour session with the help of five physiotherapists and one sports physician. The screening consisted of anthropometric measurements as well as dance specific functional tests as specified in the International Arts Injury Reporting System (IPAIRS) [6].
The anthropometric measurements included the manual muscle testing of the limbs, assessment of posture (including scapular control, iliac crest height, measurements with scoliometer), March test for sacroiliac joint mobility, calcaneal eversion, external rotation at rest and foot type.
Dancers were assessed on flexibility in the following areas: Hamstring flexibility (more than 120 degrees flexion), Thomas test, Ober's test, talocrural joint dorsiflexion (more than 5 degrees), passive great to dorsiflexion (at least 90 degrees), passive talocrural eversion (at least 5 degrees), rectus femoris flexibility (using Ely's test).
Assessment of core strength as well as dance specific tests including the sauté test, airplane test, single leg calf raisers, Romberg test, Topple test, Airplane test, Push-up and Side plank. The dancers' aerobic fitness were assessed through YMCA 3-Minute Step test which has been validated as an indirect test for aerobic fitness [7].
The dancers' quality of functional movements were assessed with the Functional Movement Assessment (FMS) [8,9]. The Functional Movement Screen is a simple codified system of assessing fundamental movement patterns. These include overhead squats, hurdle step, in-line lunge, shoulder mobility, rotatory stability, active straight leg raise and trunk stability push up. Scoring poorly in the FMS has been found to be predictive of injuries in the athletic population [10].
The subjects were monitored over twelve months for occurrence of dance injuries. The dancers would notify the investigator upon the onset of injury. With each dance injury that occurred, the dancer was interviewed and examined by the principal investigator to ensure consistency in the diagnoses. Data recorded included anatomical region and diagnoses of the injuries, the precipitating activity, venue and movement at time of injury and training hours preceding the injury. In addition, absenteeism from training as a result of the injury as well as the mode of treatment sought (if any) were documented. The dancers rated their fatigue on a analogue scale of 1 to 10 (where 1 means that he or she does not feel tired while 10 means worse tiredness imaginable). In addition, all subjects were reminded on a monthly basis to report any injuries as an additional precaution to ensure that all injuries were documented.
A total of 9 dancers were recruited, three males and six females.
All the dancers had training in multiple dance genres and had been dancing for a median of 10 (range 3-25) years. All but two had vocational dance training and all but one dancer engaged regularly in more than one genre of dance. The median training hours per week was 18 hours (range 10-24). Seven of the dancers were not employed by the company but attends company classes and rehearsals at least twice weekly and two dancers were full time professional dancers with the company.
Median age and body mass index were 27.4 years and 19.1 respectively. In the assessment for resting stance posture only one dancer had asymmetry, involving the height of the iliac crest. All dancers passed the active shoulder test for scapular control. One dancer had asymmetry of the iliac crest height. Only one dancer had positive March test on assessment of sacroiliac joints mobility (positive on both sides). Five of the dancers had calcaneal eversion of more than 5 degrees on resting stance and these were seen bilaterally. There was a wide variation in the degree of external rotation of the feet in resting stance with number to toes visible from the rear-view ranging between nil to 4 toes. Asymmetrical resting external rotation could be seen in four of the dancers with difference within one toe between sides. Two of the dancers had neutral foot posture at rest, one had cavus while the remainder had pes planus. None of the dancers had asymmetry in foot posture. One of the dancer was found to have a flat back posture on standing, one with a sway back while the rest had neutral spine.
Average passive turnout was 114 degrees with an average functional turnout of 95 degrees, and an average deficit of 9 degrees. The median Beighton score was 3 (range 0-7) with 44.4% meeting the criteria for hyper-mobility of more than four.
Further anthropometric assessment consisted of dance specific tests, assessment of tightness and manual muscle testing (Table1 and Table 2).
Table 1: Number of Dancers that Passed Dance Specific and Postural Tests. View Table 1
Table 2: Number of Dancers with Weakness on Manual Muscle Testing (MMT), n = 9. View Table 2
Dancers scored highly on the FMS (range 18-19). The most common reason for not scoring a full score for the individual stations was the detection of pain in clearing tests which screened for potential injuries. Of the tests involving laterality, only 11.1% of the results showed asymmetry.
The median result for the YMCA 3-minute step test was the good category. Two of the dancers scored below average and there was one dancer in each of the other categories (poor, average, average, above average and excellent) [11].
More than half (55.6%) had pre-existing injuries on the initial screening. Of these, 40% had two injuries, 60% had one. These included patellofemoral pain syndrome, patellar tendinitis, posterior ankle impingement and low back pain.
A total of 15 injuries were reported over a year. The majority did not result in absenteeism from dance. Only one injury resulted in cessation of dance practice for 1-2 days. Of these, 46.7% had previous injuries in the same area over the last one year (range 1-3 episodes of previous injuries) and all reported that these had recovered and been asymptomatic before the current episodes.
The anatomical distribution of these injuries is shown in (Figure 1). Two-thirds of the injuries were overuse in nature, while the rest were attributable to trauma. Most of the injuries occured during rehearsals through repetitive practice of non-stereotypical dance movements (Table 3).
 Figure 1: Anatomical distribution of dance Injuries. View Figure 1
Figure 1: Anatomical distribution of dance Injuries. View Figure 1
Table 3: Summary of Characteristics of Dance Injuries, n = 15. View Table 3
The dancers sought treatment in 26.7% of the injuries (one by sports physician, two by primary care physician and one by the masseur), while the rest of the injuries were self-managed with stretching, icing and massage.
Univariate logistic regression did no show any statistically significant correlation between the risk of injury with scores on the YMCA step test nor FMS score (p = 0.63, p = 0.44). While not reaching statistical significance, a trend towards higher fatigue rating (median 6.5) and a higher training hour (median of 18 hours of training) in the preceding week, was seen in injured dancers (Figure 2). In addition, the injuries are clustered around the months coinciding with periods of increased rehearsals in preparation for performances (Figure 3).
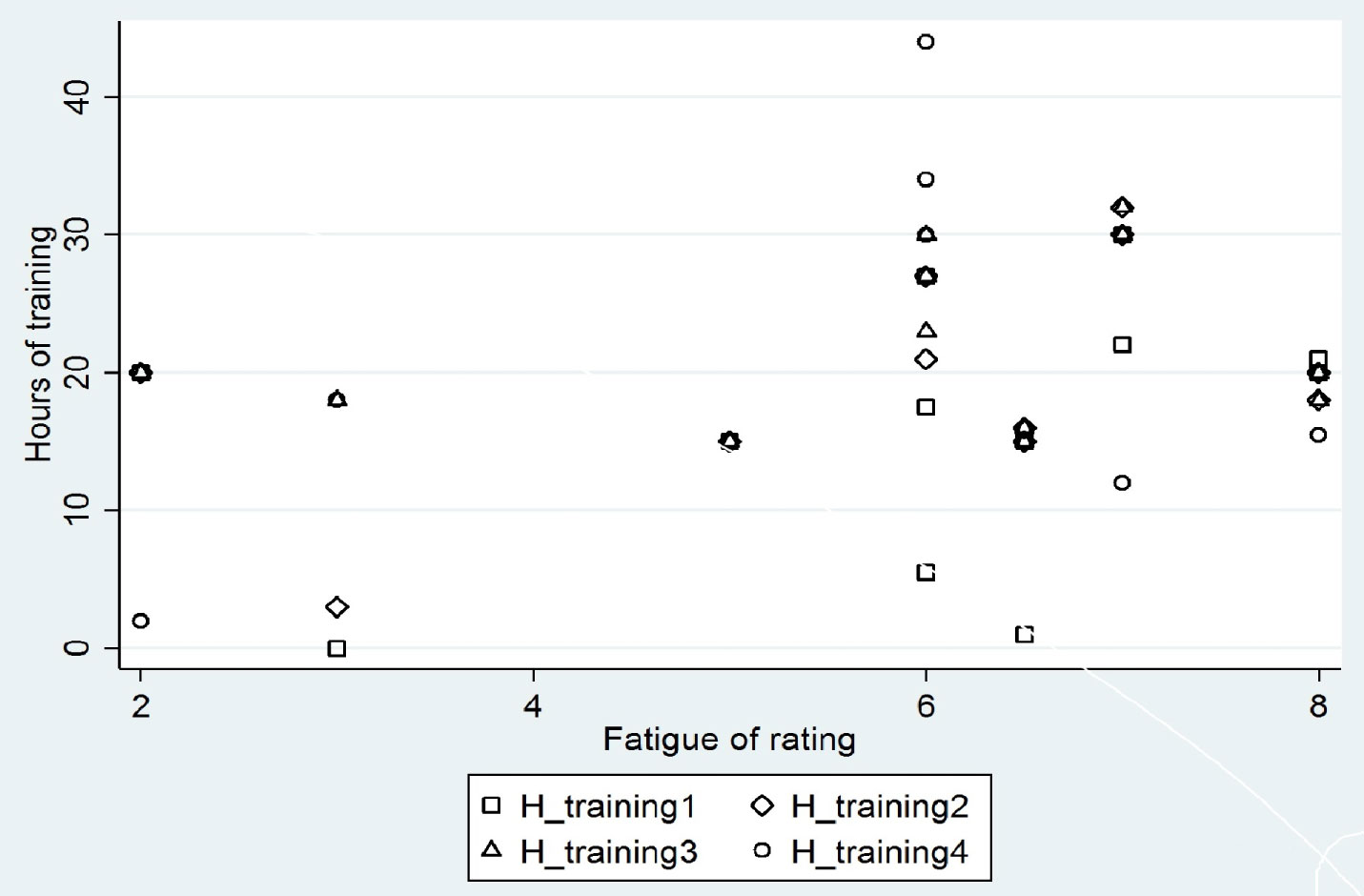 Figure 2: Scatter plot of hours of training per week of the weeks of the month preceding the injury against fatigue rating where (H_trainingn) represents the nth week of the month. View Figure 2
Figure 2: Scatter plot of hours of training per week of the weeks of the month preceding the injury against fatigue rating where (H_trainingn) represents the nth week of the month. View Figure 2
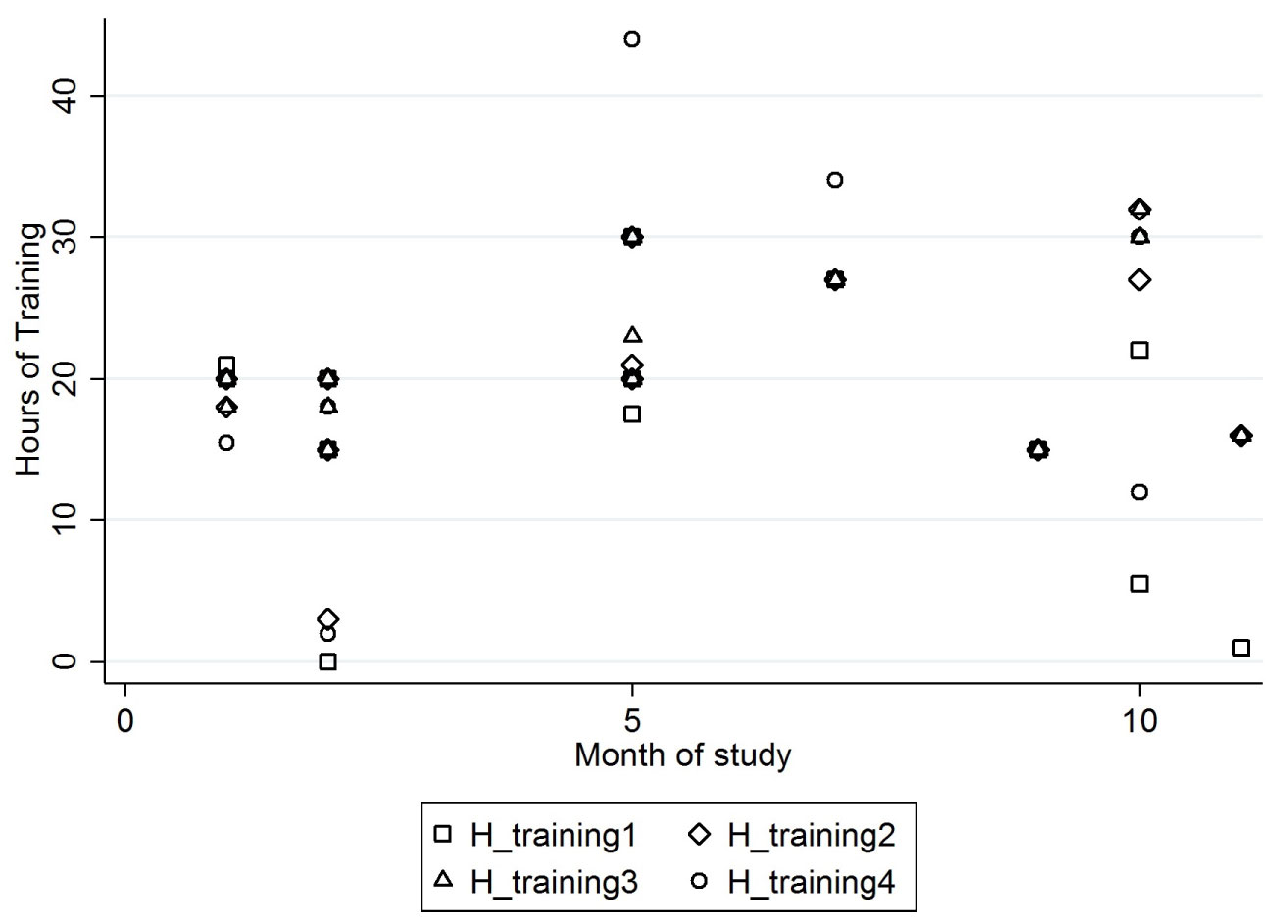 Figure 3: Scatter plot of hours of training per week of the weeks of the month preceding the injury against the month of the study (H_trainingn) represents the nth week of the month. View Figure 3
Figure 3: Scatter plot of hours of training per week of the weeks of the month preceding the injury against the month of the study (H_trainingn) represents the nth week of the month. View Figure 3
The dancers shared similar body mass index with those of their international counterparts but had lower BMI than the general population [12,13]. The prevalence of injuries at the beginning of the study were also comparable to injury patterns in other contemporary dance companies [14].
The dancers were generally symmetrical in their posture save that of external rotation of the lower limbs in resting stance. They had full and symmetrical strength although there was asymmetrical weakness of the hip strength in a minority, which could be a predisposing factor to injuries [15]. Asymmetry could result in accumulative increased tissue loading on the weaker side. Specifically, weakness in thigh strength has been associated with increased severity of injuries in ballet and contemporary dancers [16].
The difference between passive hip external rotation and active turnout (due to weakness in strength in the external rotators) has been shown to be associated with the risk of injuries in dance [17]. Weakness in hip strength can lead to compensatory movements in the other joints in the legs resulting in injuries. The discrepancy between the passive and active turnout can be reduced with dance specific training programme [18].
The proportion of dancers with hyper-mobility is comparable with that of other studies [19]. Generalised hyper mobility has been associated with an increased risk of injury in dancers [20]. While this risk factor may not be modifiable, closer monitoring of dancers with hyper-mobility could result in earlier detection and management of injuries.
The dancers performed well in dance specific functional test implying a high level of technical competency. In addition, they also scored uniformly well on the Functional Movement Screen, which contrast with data published in the athletic population where the range of score was wider [21].
Systematic review has found that scoring fourteen or below on the FMS was predictive of developing an injury [22]. As all the dancers scored above this threshold, the utility of the FMS screen aggregate score may be limited in a homogenous and experienced dance population. However, the movements assessed in FMS show low internal consistency and hence not indicators for a single factor. Hence how well the dancers performed in each of the fundamental movements may be more important than the aggregate score for injury prediction [23s].
Asymmetry on the functional movement screen has been reported in soccer players (where a leg dominance in kicking may be intrinsic to the sport), but not in cross-fit athletes where non-stereotypical movements predominate [24,25]. In the current cohort, only 11.1% had asymmetry in the test results, reflecting the lack of laterality in dance training. Inefficiencies and asymmetry in individual tests has been found to be effective in predictive for sports injuries [26].
There was a wide range of aerobic fitness in the company. Low aerobic capacity in dancers have been described in previous studies and correlated to injuries [27,28]. Despite training in the same company, the wide range of aerobic fitness highlights the importance of screening to identify members within a cohort that may benefit from supplementary training.
Cardiovascular stimulus of dance technique training is low, with a small proportion of time spent in vigorous exertion [29]. Conversely, the physiologic demands of rehearsals and performances are relatively high [1]. This discrepancy could result in fatigue and dance injuries and might also explain the propensity for injuries to occur around performance seasons [30].
Supplementary training would be necessary to improve overall aerobic fitness and health and also to delay the onset of fatigue [31]. This can be achieved with the introduction of longer exercises into conventional technical training without the need for additional sessions dedicated to aerobic training [19]. Additional physical conditioning exercise, in the form of individualised training programmes, has been shown to be effective in reducing the incidence of injuries by more than half, without adverse impact on the aesthetics of dancers [32,33].
The injury rate of this study was relatively low and the severity was mild, resulting in low absenteeism from dance participation, similar to other studies [34]. While it did not reach statistical significance, there was a trend towards increased risk of injuries when the fatigue rating went beyond six (out of ten) and when the time spent in dance training exceeded 18 hours per week. The injuries could have been linked to fatigue which is often cited as a factor in dance injuries [2]. A review of the incidences of injuries also showed a trend towards clustering of injuries in parts of the year corresponding to periods of increased training e.g. around performances (Figure 3). Closer monitoring can be instituted during these periods.
Closer inspection of the details of the injuries showed that the majority occurred during rehearsals through repetition of unfamiliar moves resulting in overuse injury rather than from trauma. This raises the possibility that these injuries could have resulted from increased tissue loading from a confluence of increased training load and inefficient movement as a result of executing novel choreographic movements.
Increased incidence of dance injuries have been observed in performing companies during tours when the accumulation of increased performances and rehearsals can result in fatigue [30]. It has been shown that fatigue has a significant impact on movement patterns in dance and provide a plausible mechanism for dance injuries [35,36].
Contrary to other studies where dance teachers and physical therapists were the first-line treatment providers, the most common source of medical care in this study was the physician [37]. Dancers often deem advice given by medical professionals without dance specific knowledge to be unhelpful [38]. Dancers would be better served by medical professionals conversant with the demands of dance and the medical issue peculiar to it [39].
As the injuries in this study result from novel choreographic movements which cannot be addressed with technical training, it might be more effective to direct injury prevention measures towards correcting physical deficiencies, such as improving resistance to fatigue through, aerobic training, strength training to redress asymmetry in strength and measures to improve recovery from training and closer monitoring of fatigue.
The screening and surveillance in this study was carried out with modest resources. A total of twenty-one man-hours were required to conduct the screening and injury surveillance over one year. Each interview, inclusive of time needed to fill up the injury reporting form, was completed in 30 minutes. Hence, the programme can be implemented without excessive demand on resources. Further savings could be made through training dancers to implement a codified screening programme [40]. Further reduction in manpower cost could be achieved in the surveillance portion by training the dancers to self-administer the injury reporting form.
The number of subjects studied was small as the result of the size of the company. This, together with the low incidence of injuries, limited the statistical inferences that could be drawn from the study. Furthermore, closer monitoring of the training load for all the dancers through the period of study, could also strengthen the inferences that can be drawn from the role of fatigue and the occurrence on injuries. Expanding the pilot study to include more dancers would increase the number of injuries studied in a more heterogenous population and improved the odds of finding associations between the dancers' characteristics and risk of injuries.
Nevertheless, the pilot project demonstrates the considerations and feasibility behind the implementation of dance injury prevention measures in Singapore.
It is feasible to implement dance specific screening and injury surveillance at the company level without large expenditure of resources. The current study highlights the poor aerobic capacity and weakness of the hip in some dancers as potential areas to address in order to reduce injuries in this cohort. Monitoring of fatigue would be useful to avoid overtraining. Closer surveillance during rehearsal would be necessary to detect injuries as these occurred mainly from repetition of non-stereotypical movements in choreography.
The author would like to thank Xiang Wei Wen and Dr Yoko Wong Kin Yoke of Tan Tock Seng Hospital for providing statistical analysis.
The author has no conflict of interest to declare.