We present the case of an active smoking 44-years-old woman (10 pack/years) diagnosed with lung adenocarcinoma T4N3M1a (stage IV) in the right upper lobe (RUL) in January 2017. She received four cycles of cisplatin-pemetrexed and radiosurgery of brain metastasis. The patient had a body mass index (BMI) of 28, with no other significant comorbidities.
In July 2017, tumoral growth with secondary airway stenosis and invasion of the superior vena cava was evidenced. Given the progression of the disease, the patient was included in a clinical trial and received six cycles of entrectinib.
In January 2018, the tumor invaded the right lower lobe (RLL) and a new brain lesion appeared in the left parietal region. Radiosurgery of the brain lesion was performed and a third line of chemotherapy with vinorelbin was started.
Despite treatment, the disease progressed and in April 2018 a fourth line of treatment with Docetaxel was initiated.
During this period, the patient attended the emergency department with cough without expectoration, tachypnea, minimal effort dyspnea and inspiratory stridor.
The chest computed tomography (CT) showed an increase in the size of the endobronchial lesion with progression towards the main carina and an obstruction of 80% of tracheal lumen (Figure 1).
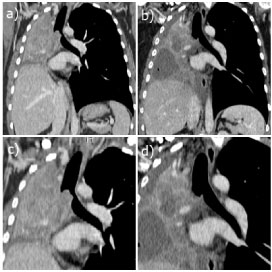 Figure 1: Coronary reconstructions of soft tissues window in chest CT (a,b) and magnified details of the trachea (c,d). Pre and after treatment studies. A complete repermeabilization of the tracheal lumen was obtained after endoscopic treatment, starting from a tracheal stenosis of approximately 80% of the lumen. View Figure 1
Figure 1: Coronary reconstructions of soft tissues window in chest CT (a,b) and magnified details of the trachea (c,d). Pre and after treatment studies. A complete repermeabilization of the tracheal lumen was obtained after endoscopic treatment, starting from a tracheal stenosis of approximately 80% of the lumen. View Figure 1
An urgent diagnosis bronchoscopy was performed, followed by a rigid bronchoscopy under general intravenous anesthesia in the operating room, showing a complete occlusion of the right main bronchus, a partial occlusion of the left main bronchus and a tracheal occlusion of approximately 80% of the lumen.
A combined technique with laser diode, diathermic handle and clamp extraction of the fragments was performed (Figure 2).
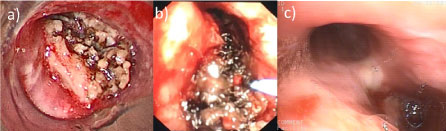 Figure 2: a) Direct visualization of the tumor through the bronchoscope; b) Tumor resection by endoscopic technique; c) Bronchoscopic control two months after tumor resection. View Figure 2
Figure 2: a) Direct visualization of the tumor through the bronchoscope; b) Tumor resection by endoscopic technique; c) Bronchoscopic control two months after tumor resection. View Figure 2
Lung cancer in patients younger than 45-years-old is a rare pathology and represents 1.2% of reported cases [1]. The case presented is unusual because of the age of the patient and the rapid progression of malignant airway obstruction despite chemotherapy treatment.
Malignant lesions that obstruct the airway are frequently associated with lung cancer or metastasis from other primary neoplasms [2].
There are several types of treatment for malignant lesions that obstruct the airway, such as: mechanical tumor resection, laser, cryotherapy, electrocautery, photodynamic therapy, brachytherapy and prosthesis adjustment [3,4].
In our case, the left bronchial tree and the tracheal lumen were completely repermeabilized after resection using a combined technique (Figure 2).
The patient did not present new episodes of dyspnea or stridor after the intervention. She was discharged the following day, after performing a revision bronchoscopy, without complications.
The rigid and flexible bronchoscopy is the first choice instrument to repermeabilized the airway and allows a safe management of the patient's ventilation.