The aim of this study was to evaluate the calcium hydroxide removal activities of Vibringe, EndoVac, passive ultrasonic and conventional needle irrigations by means of scanning electron microscope.
Seventy single-rooted human mandibular premolar teeth were used for this study. The samples were prepared with the ProTaper rotary system up to F4 and filled with calcium hydroxide. One week later, Calcium hydroxide was removed from the root canals with the several irrigation methods as follows: Vibringe (Group 1), EndoVac (Group 2), conventional needle irrigations (Group 3), passive ultrasonic (Group 4). The roots were split longitudinally and evaluated at magnifications ranging from x50 to x1000. Statistical Data were analyzed using Kruskal-Wallis and Mann-Whitney U tests.
None of the methods used in this study were able to completely remove calcium hydroxide from root canal walls. When the root canal walls were taken into consideration, there was no significant difference between Group 1, Group 2 and Group 4 (p > 0.05), but these three techniques removed more Calcium hydroxide than Group 3. When evaluated the activities of the methods in the coronal, middle and apical triple regions separately, there was a significant difference only in the Group 3 (p = 0.017) and the most residue of calcium hydroxide was found at the apical area.
Although Vibringe, EndoVac and passive ultrasonic methods were found to be more effective than conventional needle irrigations, no statistically significant difference was found between the groups.
Calcium Hydroxide, EndoVac, Passive Ultrasonic Irrigation, SEM, Vibringe
The main purpose of root canal treatment is to eliminate the existing infection in the infected root canals and to prevent subsequent infections [1]. Despite the use of different shaping techniques and the use of rotary nickel-titanium systems, due to the complex structure of the root canal anatomy, the areas which cannot be reached in the anatomical structures such as accessory and lateral canal, apical delta, canal canals may remain. In cases which root canal cleaning is not fully performed and additional disinfection applications are required, the use of canal medicaments in order to overcome this condition has been proposed [2].
Calcium hydroxide (CH) is a highly preferred canal medicament because of its many positive properties, such as its antimicrobial effect, its organic tissue solvent properties and its ability to neutralize toxins [3]. Remaining CH residues may decrease the bonding ability of root fillers to dentin and may decrease the physical properties. Therefore, CH residues need to be removed as much as possible before the root canals are permanently filled since it affect the root fillers negatively [4]. For this purpose, different irrigation solutions and many mechanical techniques have been developed.
Vibringe® (Cavex Holland BV, Haarlem, Netherlands), which is marketed by a Dutch company as a sonic washing system, is a system in which manual and sonic activation are combined. It consists of an annular plunger compatible with a 10 ml Luer-lock syringe and a wireless and rechargeable battery. By pressing the button on the inner side of the ring, vibration occurs in the needle with a vibration frequency of approximately 150 Hz. The syringe can be used in combination with various sizes of irrigation needles. In addition to the needle attached to the syringe, the irrigation solution can also be activated sonically [5].
The aim of this study was to determine the efficacy of irrigation methods which have different mechanisms for the removal of CH, which is widely used in the treatment of canal treatment. The null hypothesis was that there is not any significant differences between the irrigation systems to remove CH from root canals.
Ethical approval was given by the ethical committee of Recep Tayyip Erdogan University in Turkey (2017/07). Seventy single and flat rooted human mandibular premolar teeth which extracted for orthodontic or periodontal reasons were preferred for the study. Teeth which have caries, fractures, root canal calcification and open apex were excluded from the study. The hard and soft tissue residues on the root surfaces were cleaned with the periodontal curette and stored in 0.9% NaCl solution supported with 0.02% sodium azide until the teeth were used. The crowns of each tooth were removed from the bottom of the enamel-cement combination level with water cooling and the length of each root was fixed to 16 ± 0.5 mm. Apical openness was checked with 10 K type file (Mani Inc., Tochigi, Japan). The apical portions of the obtained roots were covered with pink wax and placed in plastic containers with polyvinyl siloxane. The preparation procedures were carried out with ProTaper Universal (Dentsply Maillefer, Ballaigues, Switzerland) file systems up to F4 file in accordance with the manufacturer's instructions. At each instrument change, root canals were irrigated with 1 mL of 2.5% NaOCl solution using a plastic syringe with a 27-gauge side-vented irrigation needle (KerrHawe SA, Bioggio, Switzerland) inserted up to the working length. A final rinse was performed with 2.5 mL of 17% EDTA followed by 2.5 mL of 2.5% NaOCl. CH powder to be used as root canal medicament was mixed with 1:1 distilled water and applied to the root canals with the help of lentulo spiral (Dyna, Bourges, France). The access cavities were sealed with a cotton pellet and a temporary filling (Coltosol; Colten, Langenau, Germany). Filled roots were stored at 37 ℃ and 100% relative humidity for 7 days. The temporary filling material and the cotton pellet was removed after the storage period.
Four different techniques were used to remove CH from the root canals. The specimens were randomly divided into four experimental groups (n = 15) considering the following irrigation/agitation methods and positive/negative control groups (n = 5).
VSI device was used together with a 27-gauge side-vented closed-ended irrigation needle (KerrHawe SA, Bioggio, Switzerland) to remove CH from the root canals. According to the manufacturer's instructions, the needle was placed 1-2 mm less than the working length. The root canals were actively irrigated with the needle by using 2.5 mL of 2.5% NaOCl and 2.5 mL of 17% EDTA for one minute by moving the needle up and forth. After every active irrigation, passive irrigation was achieved by leaving the canal undisturbed for one minute. Final irrigation was achieved by using 2.5 mL of 2.5% NaOCl for one minute followed by leaving the canal undisturbed for one minute.
First, the microcannula was placed at the working length. Canals were actively irrigated with the microcannula by using 2.5 mL of 2.5% NaOCl for one minute by moving the needle up and forth. Then, canal was left undisturbed for one minute. Thereafter, root canal was irrigated with the microcannula by using 2.5 mL of 17% EDTA for one minute and canal was left undisturbed for one minute. In the last cycle, root canal was irrigated with the microcannula by using 2.5 mL of 2.5% NaOCl for one minute and canal was left undisturbed for one minute.
2.5 mL syringe (Ayset Medical Products, Istanbul, Turkey) was used together with a 27-gauge side-vented closed-ended irrigation needle (KerrHawe SA, Bioggio, Switzerland) to remove CH from the root canals. At first, the needle was placed to the root canals 1-2 mm less than the working length. The root canals were irrigated with 2.5 mL of 2.5% NaOCl and 2.5 mL of 17% EDTA for one minute, respectively. After every active irrigation, passive irrigation was achieved by leaving the canal undisturbed for one minute as above mentioned. Final irrigation was achieved by using 2.5 mL of 2.5% NaOCl for one minute followed by leaving the canal undisturbed for one minute.
PUI was performed with a piezoelectric unit (EMS, Geneva, Sweden) and #15 stainless steel files (Nakanishi, Inc., Tochigi, Japan) were inserted into the root canal. The root canal was irrigated with 2.5 mL of 2.5% NaOCl and irrigant was ultrasonically activated for one minute moving the file up and forth without touching root walls and subsequently the canal was left with irrigant for one minute. Afterwards, root canal was irrigated with 2.5 mL of 17% EDTA for one minute and canal was left undisturbed for one minute. Finally, the canal was irrigated with 2.5 mL of 2.5% NaOCl in conjunction with ultrasonic agitation for one minute and subsequently the canal was left with irrigant for one minute.
After applying each technique, the root canals were irrigated with 2.5 mL of distilled water and wiped with sterilized with paper points. For the scanning electron microscopy (SEM) observation, in each root, parallel grooves were created in buccal and lingual regions and the root was split into two parts.
For microscopic examination, the coronal, middle and apical 1/3 regions of the root canals were marked at 0-4, 4-8 and 8-12 mm distances from the apical. Digital images at x50 and x1000 magnification were taken at the centre of root canal areas. Interpretations were performed by two independent endodontists who were experienced in the interpretation of SEM morphology by using the five-level scoring system without knowing which experimental group belonged to the samples (Table 1) [6].
Table 1: Scoring system. View Table 1
The results were statistically analyzed with Kruskal Wallis and Mann-Whitney U tests with Bonferroni correction, at 95% confidence level (P < 0.05) (SPSS 20.0 software (SPSS Inc.Chicago, IL, USA) to determine the significances between the removal techniques.
The scores for each experimental group are shown in Table 2. There was a significant difference between the positive and negative control groups (P < 0.05). Zero score was not observed in any of the groups. The results showed that there were no significant differences between the techniques of VSI, EndoVac, and PUI (P > 0.05). However, these three techniques removed more CH than CNI, significantly (P < 0.05). When the efficacy of each technique in the coronal, middle and apical regions were evaluated separately, there was a significant difference between the regions in the group of CNI (P < 0.05) and no significant difference between the regions was found in the other groups (P > 0.05).Images of calcium hydroxide residue amount in the root canals were shown in Figure 1, Figure 2, Figure 3 and Figure 4.
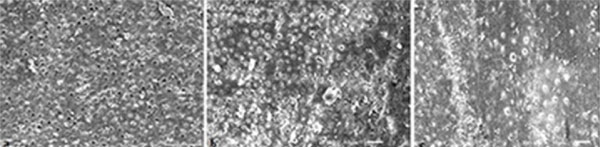 Figure 1: Calcium hydroxide residue in root canals after Vibringe sonic irrigation method (×1000 magnification) a) coronal (score 4); b) medium (score 5); c) apical (score 4).
View Figure 1
Figure 1: Calcium hydroxide residue in root canals after Vibringe sonic irrigation method (×1000 magnification) a) coronal (score 4); b) medium (score 5); c) apical (score 4).
View Figure 1
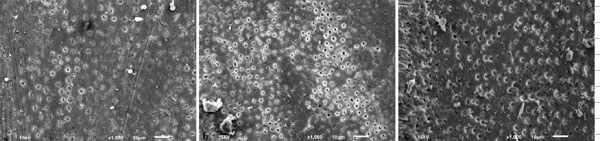 Figure 2: Calcium hydroxide residue in root canals after EndoVac sonic irrigation method (×1000 magnification) a) coronal (score 4); b) medium (score 3); c) apical (score 2).
View Figure 2
Figure 2: Calcium hydroxide residue in root canals after EndoVac sonic irrigation method (×1000 magnification) a) coronal (score 4); b) medium (score 3); c) apical (score 2).
View Figure 2
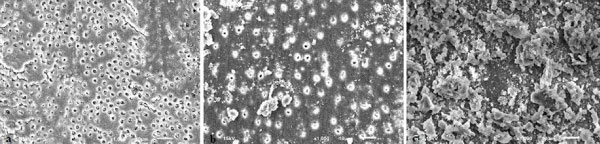 Figure 3: Calcium hydroxide residue in root canals after conventional needle irrigation method (x1000 magnification) a) coronal (score 2); b) medium (score 4); c) apical (score 5).
View Figure 3
Figure 3: Calcium hydroxide residue in root canals after conventional needle irrigation method (x1000 magnification) a) coronal (score 2); b) medium (score 4); c) apical (score 5).
View Figure 3
 Figure 4: Calcium hydroxide residue in root canals after passive ultrasonic irrigation method (x1000 magnification) a) coronal (score 1); b) medium (score 2); c) apical (score 3).
View Figure 4
Figure 4: Calcium hydroxide residue in root canals after passive ultrasonic irrigation method (x1000 magnification) a) coronal (score 1); b) medium (score 2); c) apical (score 3).
View Figure 4
Table 2: Experimental groups and scores of each root canal regions. View Table 2
Due to its antibacterial, antiresorptive and solvent properties, CH is the most preferred root canal medicament. It produces a destructive effect on bacterial membranes and walls due to high PH property, so bacterial elimination in the root canal system is provided [7]. However, the effective removal of this material as much as its use is important for treatment success. It is known that CH, which cannot be removed effectively from root canal system, inhibits penetration of root canal sealers to dentin tubules and interferes with the sealers used and affects the obstructive function by disrupting its physical properties [8]. For this reason, CH must be effectively removed before root canal obturation.
It has been reported that NaOCl is not suitable for use in the removal of CH from root canal walls due to its insufficient capacity to dissolve inorganic materials [9,10]. Therefore, in this study, it was decided to use as combined of EDTA and NaOCl irrigation agents to remove CH from the root canals [11].
When the efficacy of irrigation techniques used in this study was evaluated according to the total average scores of all root canal triple regions, the traditional needle was the most unsuccessful method in all groups. In addition, the efficacy of this method decreased from coronal to apical, and the amount of remaining CH was increased. Although traditional needle irrigation is still a widely used method, the efficacy of cleaning in the apical triple regions of the root canals is not sufficient and many previous studies supported this result [12,13]. "Vapor lock effect" phenomenon may have been effective in the emergence of this result. In this case, a complete irrigation solution flow cannot be achieved due to the air trapped between the root canals and the cannula tip, and it is difficult to perform the cleaning process [14,15].
The fact that irrigation activation methods are more effective in the coronal region can be explained by the fact that more chelator molecules can bind to calcium ions because the region is large in volume [16]. In the present study, better removal efficacy of the EndoVac system in the apical triangle rather than in the coronal may be due to better mechanical washing and turbulence in the irrigant stream with the help of negative pressure. The EndoVac system applies negative pressure rather than positive pressure, thus "Vapor Lock effect" which occurred as a natural barrier can be prevented [17]. The holes found in the microcannula cap may have been aspirated the CH residues under vacuum, thus it may have been provided more effective cleaning in the apical region. In previous studies, it was reported that EndoVac, which is a hydrodynamic irrigant activation method using negative pressure in apical, provides a high level of cleaning efficacy in root canals [18,19].
In this study, the EndoVac method was found to be more successful than the CNI technique but showed similar efficacy with VSI and PUI techniques. Some researchers have claimed that, during sonic or ultrasonic activation, the acoustic streaming and cavitation effect have disappeared in cases where the activated file leaves the irrigation solution and contacts with the gas bubble in the apex, resulting in an inadequate cleansing effect [20,21]. In the sonic systems, low displacement amplitude (1.2 ± 0.1 mm) of the tip used may cause inadequate fluid movement and low cavitation effect which is known as vapor lock effect and the low energy used is insufficient in this overcurrent [22]. In the present study, although the device tip was placed close to the apex, in the sonic and ultrasonic irrigation method, the failure may be due to vapor lock effect which occurs in the root canal system and blocks the movement of the irrigation solution. However, VSI has a non-ergonomic design with a huge integrated syringe system, it may be difficult to use for the clinician and it may shorten the activation. All these reasons may explain the failure of the canal medicament removal.
SEM evaluation method used in the study can provide to be examined only the cross-sectional of the root canals and it could not provide to be evaluated them as a whole, therefore these may have affected the results. Different methods of determination of the amount of CH remaining in the root canal walls have been carried out such as digital photographs, stereomicroscope, scanning electron microscope (SEM), computed tomography, micro-CT, spiral CT [23-25]. In this study, SEM evaluation method was performed and samples were examined under × 50 and × 1000 magnification using a scoring system similar to applied in previous studies. The scoring system has been considered to be a more reliable method compared to area calculation method because of the difficulties in distinguishing CH due to the color similarities in some parts of the dentin walls [26].
The common point in the studies done so far, as reached in this study, regardless of which method is used, the root canal medication, especially in the apical triad region cannot be cleaned sufficiently without leaving residue. This may be due to the existence of low number of dentine tubules in the apical region and existence of much more irregularities and anatomical variations.
According to current experimental study, the techniques were applied to test the irrigation systems, none of them managed to totally clean CH from the root canals. While the CNI was found to be the most unsuccessful method in all regions of the root canals, the VSI, EndoVac and PUI methods, which were used according to the manufacturer's instructions, showed similar efficacy to each other. Within the limits of this in vitro study, further clinical randomized controlled trials are needed to support the results.