Vagus nerve stimulation (VNS) is used currently in the management of drug-refractory epilepsy (DRE), and is in development for treating chronic heart failure (HF). HF is accompanied by autonomic nervous system (ANS) dysfunction, consisting of sustained sympathetic hyper-activation and withdrawal of parasympathetic tone, and associated with progressive worsening of cardiovascular (CV) function and increased morbidity and mortality. We sought to compare how VNS is utilized for DRE and may potentially be employed for HF.
A search was conducted in PubMed for all published articles using the search terms "vagus" OR "vagal" OR "VNS" AND "epilepsy", and a separate search used similar search terms AND "heart failure". Further filtering yielded the articles available as free full text, and clinical trial, prospective study, and retrospective study publications. The final selection of clinical trial/study publications in epilepsy or HF was based upon at least 3 months of follow-up and exclusion of pediatric studies. Additional information was obtained subsequently from references within these publications, and technical manuals available in the public domain.
For DRE, VNS is administered via the left cervical vagus nerve (CVN), and directed toward the central nervous system (CNS). No known biomarkers exist currently for real-time VNS adjustment. VNS is titrated empirically, using large and infrequent adjustments of VNS intensity and based upon achieving long term reduction in seizure frequency (RSF) and/or reaching the maximum tolerated VNS intensity. A significantly greater mean RSF has been observed after 3 months of VNS delivery using pulse frequency 30 Hz and duty cycle 9% (30 seconds on, 5 minutes off) when compared to using 1 Hz and duty cycle 14% (30 seconds on, 3 minutes off). A further reduction of mean RSF has been observed after 12 months by increasing the pulse frequency at 3 months from 1 to 30 Hz.
For HF, VNS has been administered via the left or right CVN, targeting both the CNS and/or peripheral hierarchical autonomic reflex arcs that control cardiovascular function. Real-time changes in heart rate dynamics (HR and HR variability) have served as a biomarker of ANS engagement (ANSE) for titration. Titration to ANSE has been completed in 2.5 (median; range 1.6-3.6) months using 10 Hz and duty cycle 23% (18 seconds on, 1 minute off), using smaller and more frequent adjustments of VNS intensity, and has been associated with significant improvements after 6 months in HR, HR variability, CV function, and HF symptoms. Use of 1 Hz may have less clinical efficacy than occurs with a higher pulse frequency, however, intolerable side effects have occurred before ANSE using 20 Hz.
Neuromodulation for the treatment of epilepsy and HF is not a one-size-fits-all therapy. The magnitude of long term reduction of seizure frequency in DRE, and improvements in function and symptoms in HF, may have a potential dose-dependent relationship to the intensity of VNS delivery. However, VNS for these disorders differs in neurologic targets, the technology platforms and paradigms used for titration, and the time and the frequency needed for up-titrating VNS.
Autonomic nervous system, Autonomic regulation therapy, Neuromodulation, Vagus nerve stimulation
ANS: Autonomic Nervous System; ART: Autonomic Regulation Therapy; HF: Chronic Heart Failure; CNS: Central Nervous System; CV: Cardiovascular; CVN: Cervical Vagus Nerve; DRE: Drug-Refractory Epilepsy; GDMT: Guideline Directed Medical Therapy; HFrEF: Heart Failure with Reduced Left Ventricular Ejection Fraction; HR: Heart Rate; VNS: Vagus Nerve Stimulation
Vagus nerve stimulation (VNS) for neuromodulation [1] is used currently for the management of patients with drug-refractory epilepsy [2,3], and is an investigational therapy being evaluated in patients with chronic heart failure (HF). HF is known to be accompanied by autonomic dysfunction that results in sympatho-vagal imbalance with sustained sympathetic hyperactivation and withdrawal of parasympathetic tone [4-6]. This results in progressive cardiac dysfunction that is manifested as worsening HF [7-10] with increased risk of mortality and morbidity [11,12].
Although remarkable progress has been made to correct the sympatho-vagal imbalance in HF by blocking the deleterious effects of sympathetic hyperactivation with beta-blockers and andrenin-angiotensin-aldosterone system (RAAS) inhibitors with considerable success, HF remains a progressive, deteriorating condition and there are as yet no approved therapies to improve parasympathetic tone. To overcome this gap, VNS is in development as a possible therapeutic option.
For epilepsy, VNS is utilized to decrease the frequency of seizures [2]. In HF, early data shows that VNS potentially improves symptoms, cardiac function, and quality of life, and its effects on long-term outcomes including mortality and hospitalization for heart failure are being assessed [13]. In this article, we describe how VNS has been deployed for its intended objectives in the treatment of epilepsy and HF.
A search was conducted in PubMed for all published articles using the search terms "vagus" OR "vagal' OR "VNS" AND "epilepsy", and a separate search used similar search terms AND "heart failure". Further filtering yielded the articles available as free full text, and clinical trial, prospective study, and retrospective study publications. The final selection of clinical trial/study publications in epilepsy or HF was based upon at least 3 months of follow-up and exclusion of pediatric studies and redundancies. Additional information was obtained subsequently from references within these publications, and technical manuals available in the public domain.
The consort diagrams in Figure 1 provide the search results, and Table 1 and Table 2 provide an overview of the clinical studies that were identified for DRE and HF, respectively.
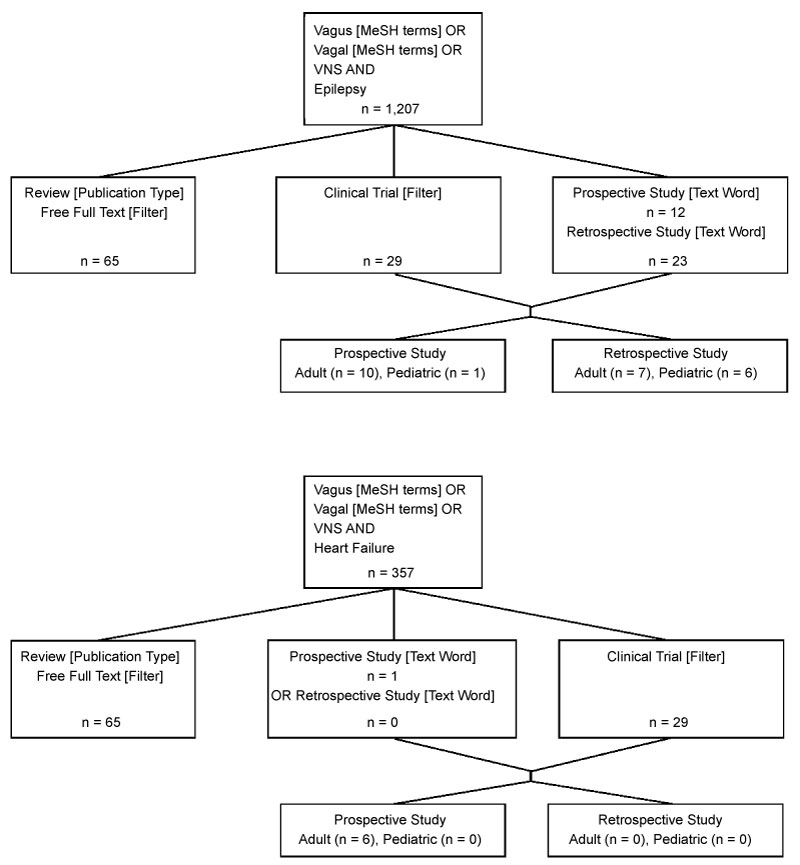 Figure 1: CONSORT diagrams of search results for DRE and HF. View Figure 1
Figure 1: CONSORT diagrams of search results for DRE and HF. View Figure 1
Table 1: Clinical studies of VNS in patients with drug-refractory epilepsy. View Table 1
Table 2: Clinical studies of VNS in patients with heart failure and reduced ejection fraction. View Table 2
VNS is delivered utilizing a pulse generator, an electrode lead that surrounds the cervical vagus nerve (CVN), and an external programming system used to change the generator settings for stimulating the vagus nerve. The electrode lead requires no intraoperative mapping for placement. The generator and lead deliver electrical stimulation to axons that comprise the CVN; this includes approximately 80% afferent and 20% parasympathetic preganglionic efferent projections [37-39].
VNS parameters include intensity of the current stimulus, its polarity, and mode of delivery. VNS intensity comprises the combination of the pulse amplitude, pulse frequency, pulse duration (width), and duty cycle. The duty cycle consists of a period of VNS ("on-time") alternating with a period of no stimulation ("off-time"), is measured by dividing the duration of the on-time by the total cycle duration (i.e., on-time plus off-time) and is repetitive over time. The mode of delivery may be closed-loop or open-loop. Closed-loop delivery comprises VNS that occurs only in response to an external stimulus. Open-loop delivery comprises VNS that occurs without any dependence on detection of an external stimulus (Figure 2).
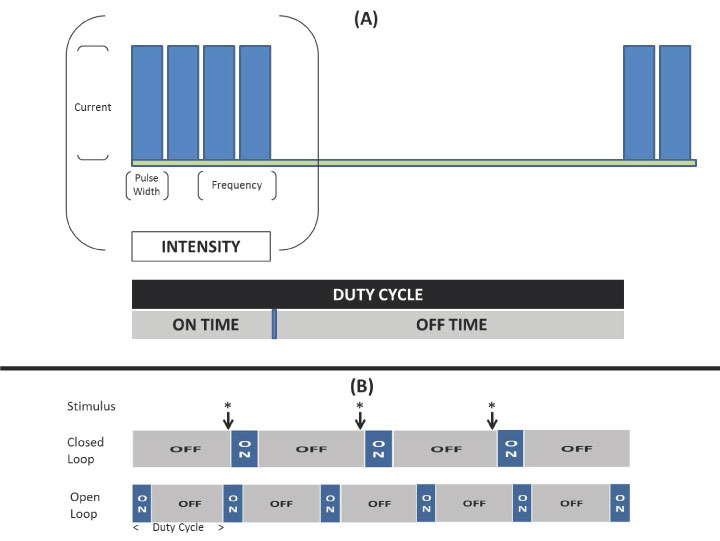 Figure 2: VNS delivery includes its intensity (a combination of pulse amplitude, pulse frequency, and pulse duration) and duty cycle (Panel A). The mode of delivery may be open-loop or closed loop (Panel B). View Figure 2
Figure 2: VNS delivery includes its intensity (a combination of pulse amplitude, pulse frequency, and pulse duration) and duty cycle (Panel A). The mode of delivery may be open-loop or closed loop (Panel B). View Figure 2
For epilepsy, VNS is administered using open-loop delivery to the left cervical vagus nerve, and directed preferentially toward the central nervous system (CNS) by orienting the cathodic electrode toward the brain. There are as yet no known biomarkers that have been established for real-time titration of VNS for DRE into a therapeutic range. For this reason, a change in seizure frequency is the metric of choice to guide VNS titration [1-3].
The reduction of long term seizure frequency appears to be associated with the VNS intensity that is utilized. A significantly greater reduction in seizure frequency after 3 months has been observed with VNS delivery at "high" intensity when compared to VNS delivered at a "low" intensity ("high": Pulse frequency 30 Hz; duty cycle 9% [30 seconds on, 5 minutes off]; current 0.25-2.5 mA; "low": Pulse frequency 1 Hz; duty cycle 14% [30 seconds on, 3 minutes off]; current 0.25-2.5 mA) [16,18]. Adjustment of VNS delivery to "high" intensity after 3 months at "low" intensity has been associated at 12 months with a significant subsequent reduction in mean seizure frequency [20], and a significant reduction in median seizure frequency has been reported when "high" intensity includes a duty cycle > 22% or a duty cycle with an off time of 1.1 minutes [40].
A clinical paradigm for VNS titration has evolved from these observations. Initially, pulse widths of 250 or 500 microseconds, and a pulse frequency of 30 Hz signal frequency are typically utilized while the output current is increased in 0.25 mA increments over the first 12 weeks of VNS Therapy. During this time, the duty cycle is 10% (i.e., 30 seconds on, 5 minutes off). After the device output current reaches 1.5 to 1.75 mA, the duty cycle off-time is reduced, and seizure activity is monitored for an additional three months before additional adjustments are made [41,42].
Several alternative approaches have been explored for delivering VNS for the treatment of HF. VNS has been administered via the left or right CVN, and the technology platforms and methods for HF have differed from that for epilepsy (Figure 3A) [31-33,36,43-45]. VNS polarity and software are configured to direct stimulation toward both the CNS and the periphery. The goal of VNS titration has been to objectively confirm autonomic engagement for cardiac control using sinoatrial node behavior as a biomarker. Changes in heart rate and heart rate variability have been targeted to confirm adequate autonomic engagement [46]. Smaller and more frequent adjustments of VNS are employed to achieve autonomic engagement using a minimum effective VNS intensity, which allows titration to be completed in a shorter period of time (Table 2).
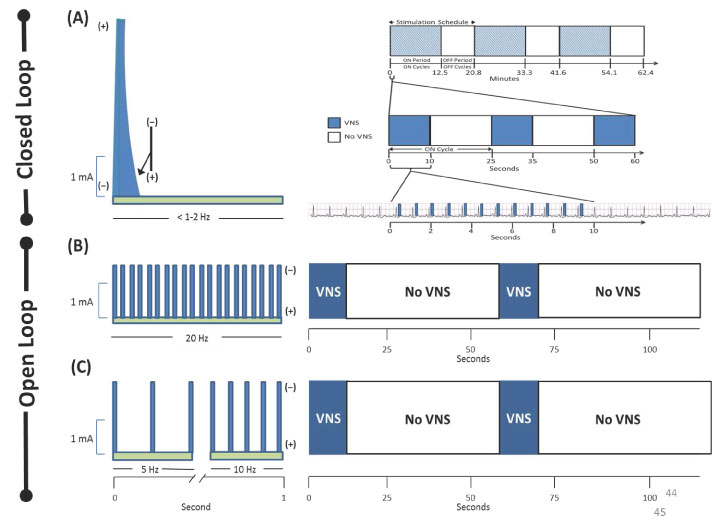 Figure 3a: Comparison of pulse frequencies, polarities, and duty cycles used for VNS delivery for the treatment of heart failure in INOVATE-HF (Panel A) [36], NECTAR-HF (Panel B) [33], and ANTHEM-HF (Panel C) [32,34]. The mode of VNS delivery was closed-loop in INOVATE-HF, and open-loop in the other studies. INOVATE-HF utilized a repetitive stimulation schedule for VNS delivery consisting of ON Cycles followed by OFF Cycles. Each cycle comprised an ON Time followed by an OFF Time. ON Cycles delivered VNS for detected R-waves during the ON Time and no VNS during the OFF Time. OFF Cycles delivered no VNS during the ON Time or the OFF Time. As an example, nominal stimulation schedule could be programmed to have a sequence of 30 ON Cycles followed by 20 OFF Cycles, a total duration of 25 seconds for each cycle, and delivery of a single VNS pulse for each detected R-wave during the first 10 seconds of each ON Cycle [38]. Administration of a single VNS pulse following at most 25% of detected R-waves would yield VNS delivery with a pulse frequency of < 1 when administered during heart rates of 56-130 beats per minute. Administration of three VNS pulses as the maximum number of pulses allowable would yield a pulse frequency of < 2 Hz. View Figure 3a
Figure 3a: Comparison of pulse frequencies, polarities, and duty cycles used for VNS delivery for the treatment of heart failure in INOVATE-HF (Panel A) [36], NECTAR-HF (Panel B) [33], and ANTHEM-HF (Panel C) [32,34]. The mode of VNS delivery was closed-loop in INOVATE-HF, and open-loop in the other studies. INOVATE-HF utilized a repetitive stimulation schedule for VNS delivery consisting of ON Cycles followed by OFF Cycles. Each cycle comprised an ON Time followed by an OFF Time. ON Cycles delivered VNS for detected R-waves during the ON Time and no VNS during the OFF Time. OFF Cycles delivered no VNS during the ON Time or the OFF Time. As an example, nominal stimulation schedule could be programmed to have a sequence of 30 ON Cycles followed by 20 OFF Cycles, a total duration of 25 seconds for each cycle, and delivery of a single VNS pulse for each detected R-wave during the first 10 seconds of each ON Cycle [38]. Administration of a single VNS pulse following at most 25% of detected R-waves would yield VNS delivery with a pulse frequency of < 1 when administered during heart rates of 56-130 beats per minute. Administration of three VNS pulses as the maximum number of pulses allowable would yield a pulse frequency of < 2 Hz. View Figure 3a
Some studies have evaluated VNS for HF utilizing open-loop stimulation in both afferent (toward the brain) and efferent direction (toward peripheral hierarchical autonomic reflex arcs) to control cardiovascular function [32,33]. Use of a pulse frequency of 20 Hz (Figure 3A, Panel B) has been reported to cause significant off-target effects that have made it intolerable to up titrate the stimulation current sufficiently to engage the ANS acutely, to achieve any significant long term changes in heart rate (HR) or parameters of HR variability that would be indicative of autonomic engagement, or to attain sufficient subsequent improvement in signs and symptoms of HF [33,35].
An alternative approach has used closed-loop stimulation that requires implantation of a right ventricular (RV) pacemaker lead for synchronizing VNS delivery with RV depolarizations [31,36,44]. This technology delivers VNS using a quasi-trapezoidal, charge balanced, asymmetric current pulse. An initial high-amplitude anodal phase is employed in an attempt to produce electrophysiological conduction block in the afferent direction. This is followed by a cathodic efferent phase with a current that is limited to an amplitude that is 5% of the amplitude of the initial phase [47]. VNS occurs intermittently, based on a repetitive and complex stimulation schedule (Figure 3A, Panel A) that administers VNS following at most 25% of detected R-waves [31,38]. This approach, coupled with the nominal delivery of a single pulse and no more than three pulses per sensed R-Wave for heart rates in the range of 56-130 beats/minute, administers VNS with a pulse frequency of less than 1-2 Hertz. To date, no long term changes in heart rate, consistent with modulation of the autonomic nervous system, has been observed with this technique [36].
In a third approach, VNS of the left and right cervical vagus have been compared in patients with HF and reduced left ventricular ejection fraction (HFrEF) [32]. The pulse frequencies for VNS in this study and its long term follow-up were selected to be similar to the spontaneous frequency observed in the efferent fibers of the vagal trunk (Figure 3A, Panel C) [48]. In this study, VNS successfully engaged the ANS in all patients while they were receiving standard of care treatment with Guideline Directed Medical Therapy (GDMT), as indicated by real-time changes in HR [49,50]. There was also a significant long term decrease in 24-hour heart rate and a significant increase in 24-hour heart rate variability, which are compatible with a sustained improvement in autonomic tone. VNS delivered in this manner was associated with significant increases when compared to baseline in left ventricular ejection fraction, 6-minute walk distance, NYHA classification, and quality of life [32]. A post-hoc analysis has suggested that the greater magnitudes of clinical improvement in this study could be related to the differences in the technology platform and method that were used for VNS delivery when compared to the other two approaches (Figure 3B) [51]. A control arm of GDMT alone was not included in the ANTHEM-HF Pilot Study, however, therefore the overall effects that were observed may not have been solely attributable to ART alone. It is possible that at least some of the clinical improvements may have been related to the open label nature of the study and/or a Hawthorne effect that may have affected the more subjective assessments. Nevertheless, the overall direction of changes that have been observed in patient symptoms and function after 6, 12, 24, and 42 months have been encouraging [32,34,52]. Confirmation of these findings are being investigated further in a larger, multi-center, randomized, placebo controlled study [13].
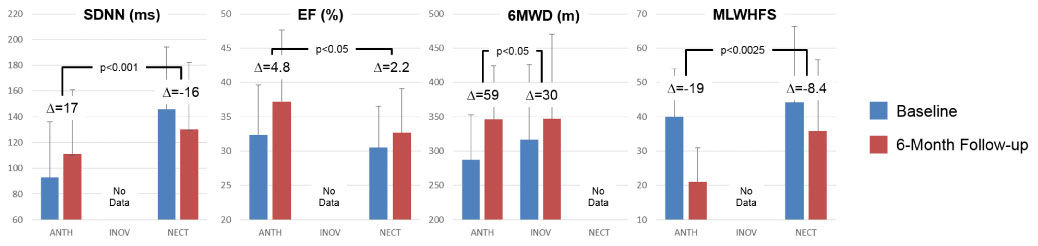 Figure 3b: Symptomatic and functional responses to VNS in INOVATE-HF, NECTAR-HF, and ANTHEM-HF. During chronic VNS in patients with HFrEF, heart rate and heart rate variability (SDNN) improved only in ANTHEM-HF. Significantly greater responses to VNS were observed in cardiac function & HF symptoms in ANTHEM-HF when compared to INOVATE-HF and NECTAR-HF. View Figure 3b
Figure 3b: Symptomatic and functional responses to VNS in INOVATE-HF, NECTAR-HF, and ANTHEM-HF. During chronic VNS in patients with HFrEF, heart rate and heart rate variability (SDNN) improved only in ANTHEM-HF. Significantly greater responses to VNS were observed in cardiac function & HF symptoms in ANTHEM-HF when compared to INOVATE-HF and NECTAR-HF. View Figure 3b
Figure 4 illustrates the methods used to deliver VNS in patients with epilepsy and patients investigated in the ANTHEM-HF Pilot Study. VNS for HF utilized a relatively larger duty cycle, a lower pulse frequency, and an output current that on average was higher than that used for epilepsy.
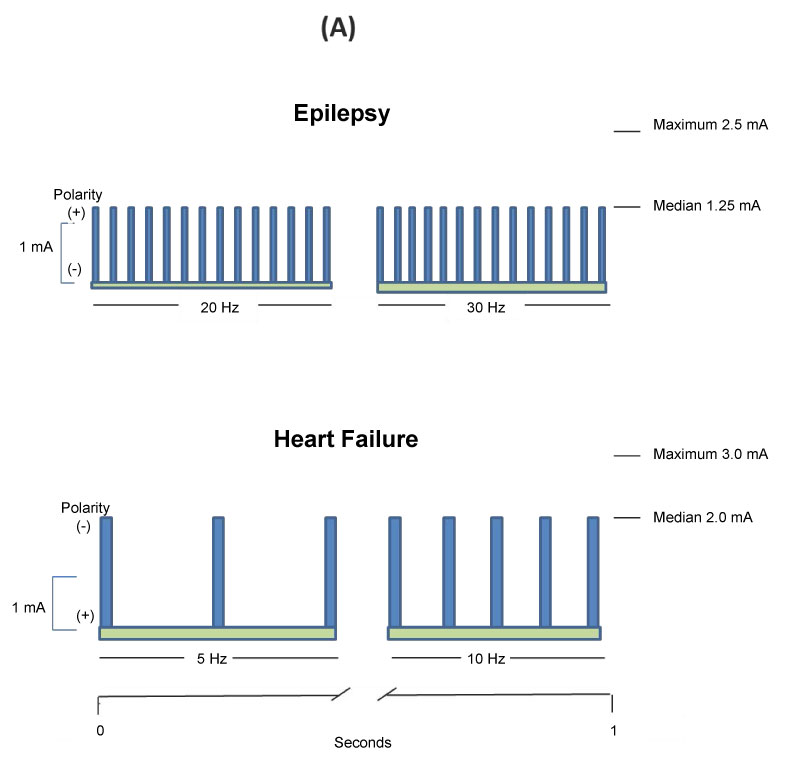 Figure 4:a Comparison of pulse frequencies, polarities, and amplitudes for VNS delivery in the treatment of epilepsy and as utilized in ANTHEM-HF. View Figure 4a
Figure 4:a Comparison of pulse frequencies, polarities, and amplitudes for VNS delivery in the treatment of epilepsy and as utilized in ANTHEM-HF. View Figure 4a
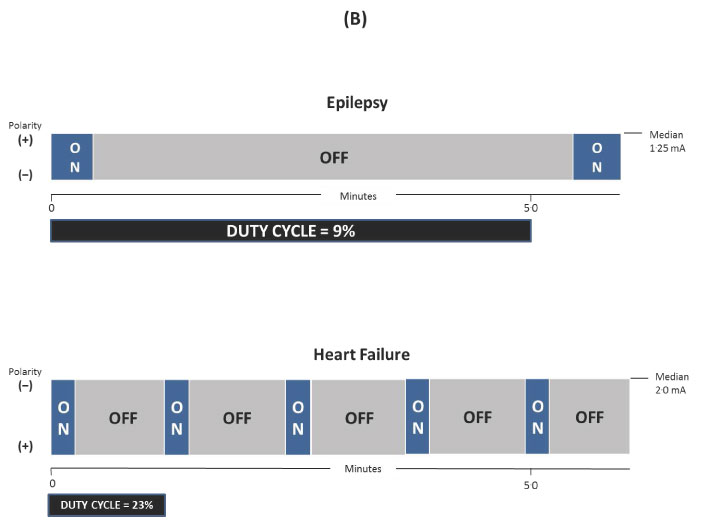 Figure 4b: Comparison of duty cycles for VNS delivery in the treatment of epilepsy [41,42] and as utilized in ANTHEM-HF and its long-term followup [32,34,52]. View Figure 4b
Figure 4b: Comparison of duty cycles for VNS delivery in the treatment of epilepsy [41,42] and as utilized in ANTHEM-HF and its long-term followup [32,34,52]. View Figure 4b
The hallmark of epilepsy is recurrent seizures, and it is the third most common neurological disorder in the world. Medications are inadequate for seizure control in up to 40% of afflicted patients [53]. Surgery may reduce or eliminate seizures in as many as 60% of patients with drug-refractory epilepsy. However, the remainder of patients continue to experience seizures that adversely impact their ability to conduct usual activities of daily living [54,55]. Long-term consequences can include increased seizure severity [56], seizure-related injuries [57], increased healthcare utilization [58], and increased mortality.
The hallmarks of HF include progressive deterioration of cardiac function, worsening symptoms that ultimately impair the ability to conduct activities of daily living, and a reduced life-span. Despite the remarkable progress that has been made in the use of pharmacologic therapy and devices for HF, the overall prognosis of patients with HF still remains poor. In many patients, cardiac dysfunction and clinical manifestations of heart failure persist and worsen in conjunction with chronic dysregulation of the ANS [10].
In the more established domain of VNS for the treatment of epilepsy, the clinical benefits of VNS have been associated with interaction with the CNS [1]. The locus coeruleus and the dorsal raphe nucleus appear to play prominent roles in putative effects. Both of these have widespread projections to the brain and spinal cord, and release neuromodulators with robust antiepileptic effects during acute and chronic VNS. VNS-induced seizure suppression is abolished when they are interrupted [59].
VNS for HF is based on the hypothesis that down-regulation of the parasympathetic nervous system contributes to the progression of HF. VNS may benefit patients with HF by increasing parasympathetic activity, and a different paradigm is required for VNS administration and titration to achieve these objectives. Experimental studies have confirmed that VNS exerts anti-adrenergic effects by pre- and post-junctional interactions at end-terminus projections onto cardiomyocytes, and restoring synaptic efficacy within the intrinsic cardiac nervous system [60-63]. The objective of VNS for HF is the engagement of neurologic targets that include the CNS and ANS at multiple levels (Figure 5) [64-67]. Reaching a critical level of vagal stimulation appears to be essential in promoting beneficial modulation of central and peripheral autonomic nervous system (ANS) activity [46]. In order to achieve the appropriate level of autonomic engagement in a timely manner with the minimum effective VNS intensity, frequent programming and gradual adjustments of VNS pulse amplitude, pulse width, and pulse frequency (referred to as "titration") are required. VNS can be titrated to produce an immediate, relatively small change in beat-to-beat distribution of R-R intervals during the ON time of the VNS duty cycle. This change has been observed to correlate with the current amplitude of VNS. During titration of right CVNS, a strong correlation has been observed between stimulus intensity and a Poincaré map parameter of standard deviation, which is associated with high-frequency heart rate variability. The effect of VNS on instantaneous heart rate has consisted of a shift in the centroid of the beat-to-beat cloud distribution of R-R intervals (Figure 6), with a tight coupling in beat-to-beat dynamics during VNS stimulation that has been directly related to stimulation intensity. This has provided a useful measurement for confirming an appropriate level of autonomic engagement [50]. This coupling has been achieved and maintained without any long-term side effects [50,68], and has been associated with significant and clinically meaningful improvements in HF symptoms, exercise capacity, and cardiac function [32,34,52].
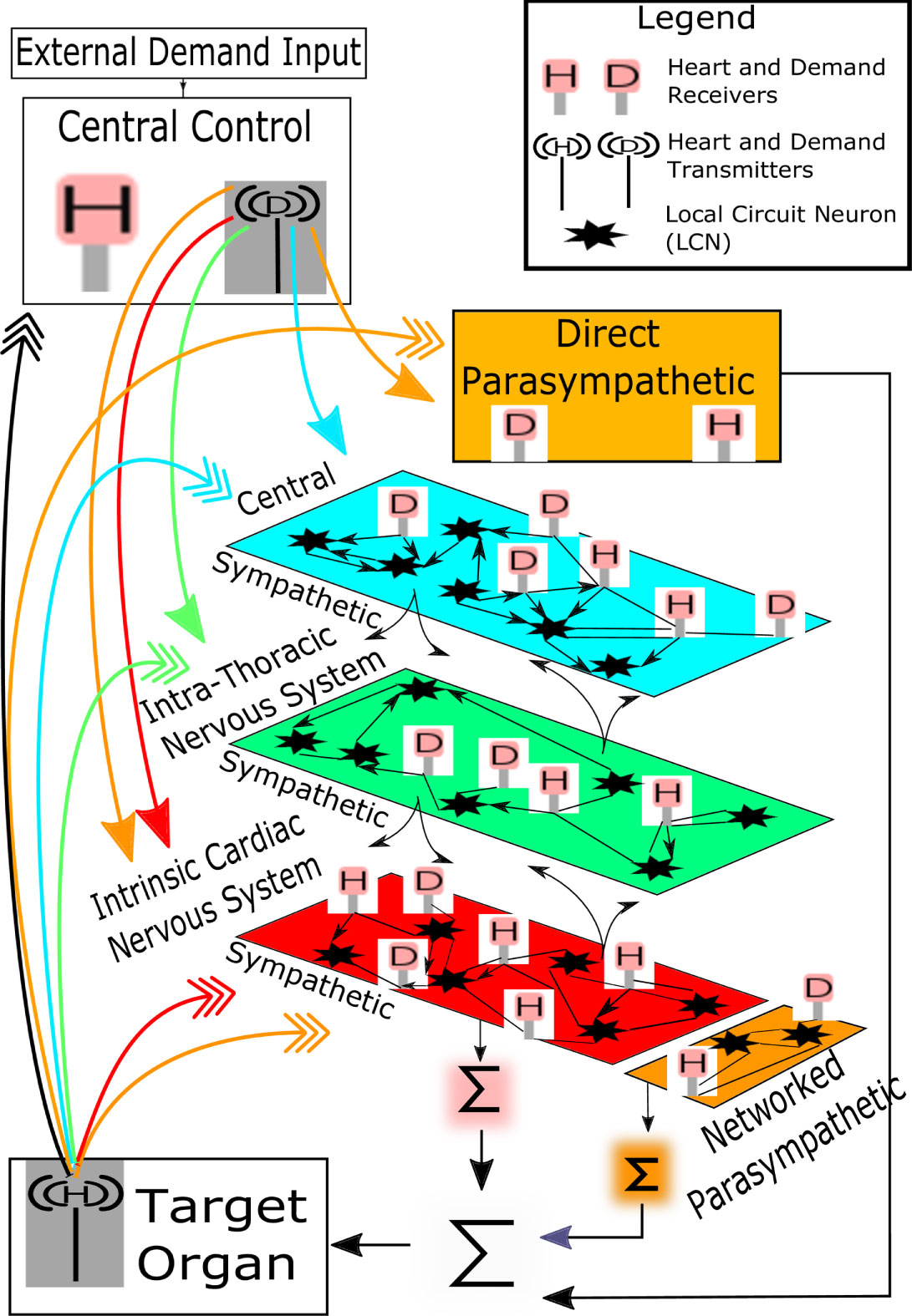 Figure 5: Cardiac function and homeostasis includes processes within the central nervous system as well as local circuit neurons for networked control within the peripheral nervous system. Network interactions occur within the local circuit neural (LCN) populations. These integrate activities within and between peripheral ganglia and the central nervous system subserve reflex control of the heart. The intrinsic cardiac nervous system possesses sympathetic (Sympath) and parasympathetic (Parasym) efferent post-ganglionic neurons, local circuit neurons, (LCN) and afferent (Aff.) neurons. The intrathoracic extracardiac nervous system is comprised of ganglia containing afferent neurons, LCN, and sympathetic efferent post-ganglionic neurons. Cardiovascular heart rate and demand inputs are conveyed centrally via dorsal root (DRG), nodose, and petrosal ganglia subserving spinal cord (C-cervical, T-thoracic), brainstem, and higher center reflexes for hemostatic maintenance. From Kember G. PLosONE 2017 (with permission) [65]. View Figure 5
Figure 5: Cardiac function and homeostasis includes processes within the central nervous system as well as local circuit neurons for networked control within the peripheral nervous system. Network interactions occur within the local circuit neural (LCN) populations. These integrate activities within and between peripheral ganglia and the central nervous system subserve reflex control of the heart. The intrinsic cardiac nervous system possesses sympathetic (Sympath) and parasympathetic (Parasym) efferent post-ganglionic neurons, local circuit neurons, (LCN) and afferent (Aff.) neurons. The intrathoracic extracardiac nervous system is comprised of ganglia containing afferent neurons, LCN, and sympathetic efferent post-ganglionic neurons. Cardiovascular heart rate and demand inputs are conveyed centrally via dorsal root (DRG), nodose, and petrosal ganglia subserving spinal cord (C-cervical, T-thoracic), brainstem, and higher center reflexes for hemostatic maintenance. From Kember G. PLosONE 2017 (with permission) [65]. View Figure 5
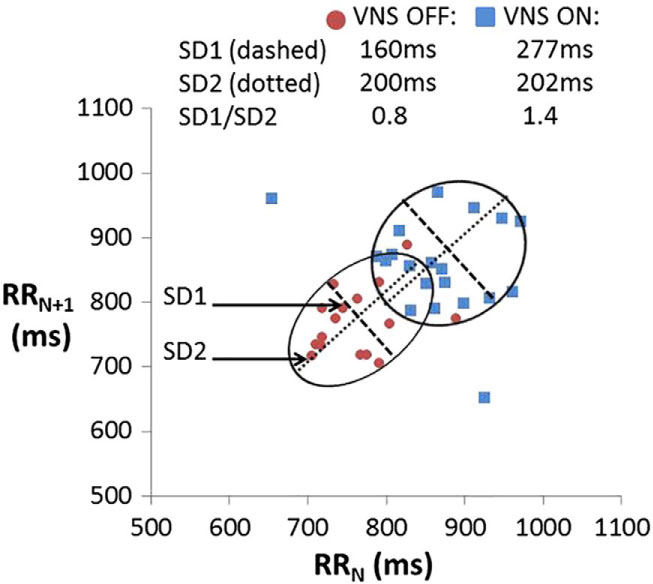 Figure 6: Quantitative beat-to-beat (RR) analysis of heart rate dynamics using the Poincaré method. There is a close coupling between the "ON" periods of VNS stimulation in humans with the beat-to-beat dynamics. During the right-sided VNS "ON" time, there is an upward shift and expansion of the beat-distribution cloud, reflected in an increase in SD1, and an increase in the average R-R intervals, consistent with an increase in parasympathetic input. Abbreviations: ms: Milliseconds; RRN: The time between two successive R-waves (ventricular electrograms); RRN+1: The time between the next two successive R-waves; SD1: Instantaneous beat-to-beat variability in successive RR intervals; SD2: Standard deviation of continuous beat-to-beat R-R interval variability; SD1/SD2: A measure of autonomic balance with higher values correlating with vagal tone preponderance. From Libbus I. J Electrocardiol 2017 (with permission) [50]. View Figure 6
Figure 6: Quantitative beat-to-beat (RR) analysis of heart rate dynamics using the Poincaré method. There is a close coupling between the "ON" periods of VNS stimulation in humans with the beat-to-beat dynamics. During the right-sided VNS "ON" time, there is an upward shift and expansion of the beat-distribution cloud, reflected in an increase in SD1, and an increase in the average R-R intervals, consistent with an increase in parasympathetic input. Abbreviations: ms: Milliseconds; RRN: The time between two successive R-waves (ventricular electrograms); RRN+1: The time between the next two successive R-waves; SD1: Instantaneous beat-to-beat variability in successive RR intervals; SD2: Standard deviation of continuous beat-to-beat R-R interval variability; SD1/SD2: A measure of autonomic balance with higher values correlating with vagal tone preponderance. From Libbus I. J Electrocardiol 2017 (with permission) [50]. View Figure 6
Past and current development of implantable and non-implantable VNS has also occurred for other indications such as major depression, anxiety, arrhythmias, cluster headache, cognition and brain injury, inflammation and autoimmune diseases, ischemia and myocardial infarction, migraine, obesity, pain, and rheumatoid arthritis [69,70]. This report was not intended to be an exhaustive review of all of these conditions, other conditions that might be amenable to neuromodulation, or alternative methods that might be used for modulating the nervous system. The objective of this report was to describe VNS as it is currently approved for use in the management of DRE, and to compare this with the more recent use of VNS in patients with HFrEF, in order to illustrate how VNS for these disorders differs in neurologic targets, the technology platforms and paradigms used for titration, and the time and the frequency needed for up-titrating VNS to achieve its intended therapeutic effects.
Neuromodulation for the treatment of epilepsy and HF is not a one-size-fits-all therapy. The magnitude of long term reduction of seizure frequency in DRE, and improvements in function and symptoms in HF, seem to have a potential dose-dependent relationship to the intensity of VNS that is utilized. However, the delivery of VNS for these disorders differs in neurologic targets, the technology platforms and paradigms used for titration, and the time and the frequency needed for up-titrating VNS.
Because no biomarker currently exists to guide VNS titration for DRE, VNS titration is based upon observing a reduction in seizure frequency or reaching the maximum tolerated VNS intensity. Increasing data suggest that changes in heart rate dynamics may serve as a biomarker for confirming satisfactory ANS engagement during VNS up-titration to ameliorate HF. The minimum effective VNS intensity that achieves this engagement may be sufficient, and the completion of up-titration is possible in a shorter period of time if smaller and more frequent adjustments of VNS intensity are used. Strong and favorable clinical responses were observed with the approach used in the ANTHEM-HF Pilot Study. A similar paradigm is being tested in an international, multicenter, randomized controlled study of right CVNS to evaluate the role of ART in patients with HFrEF.
No funding was provided and no medical writer was used for the preparation of this manuscript. I. Anand and M. Konstam are contracted to LivaNova as cardiovascular consultants, and J. Ardell is contracted to LivaNova as a neurocardiology consultant. I. Libbus and L. DiCarlo are employees and shareholders of LivaNova USA Incorporated. M. Konstam is the Chair, and I. Anand and D. Mann are members, of the Steering Committee for the ANTHEM-HFrEF Pivotal Study.
All authors contributed equally to the writing of this manuscript, had full access to all of the sources for this article, and shared final responsibility for the decision to submit it for publication.
None.