The case of a 52-year-old female patient is reported who suffered aborted sudden cardiac arrest, got layman’s resuscitation, and then defibrillation into normal sinus rhythm with temporary right precordial ST segment elevation.
The patient was admitted to hospital, the diagnosis of early-stage arrhythmogenic cardiomyopathy by ECG, echocardiography and left ventricular, right ventricular and coronary angiography was made. Echocardiography findings revealed dilatation of the right ventricular outflow tract and the in flow tract. Right ventricular angiography revealed loss of trabecular structure of the inferior wall and the apiex of the right ventricle. ECG revealed localized right precordial QRS prolongation and T-wave in version in V1 and V2. Electrophysiological testing could exclude inducible ventricular tachycardian or ventricular fibrillation. At the end of EP testing an ajmaline challenge was performed with the induction of low voltage type I Brugada ECG, QRS fragmentation in lead V2 and the phenomenon of localized right precordial QRS prolongation after ajmaline injection (Figure 1). Laboratory findings such as potassium and calcium were within normal range. The past history of the patient was uneventful, family history showed no clinical events. The patient refused genetic testing.
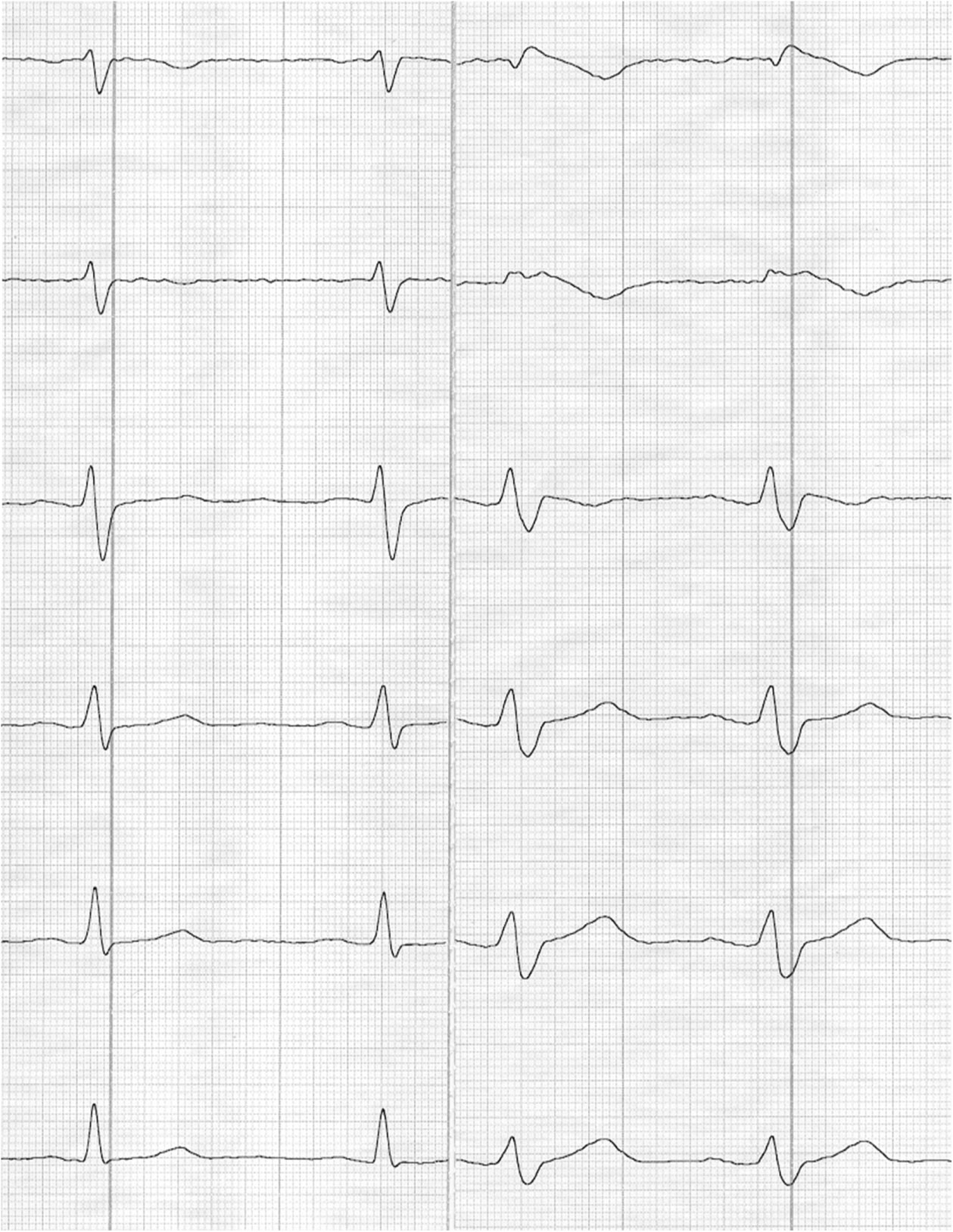 Figure 1: Documentation of Brugada ECG in precordial leads at rest (left side) and after ajmaline challenge (right side).
View Figure 1
Figure 1: Documentation of Brugada ECG in precordial leads at rest (left side) and after ajmaline challenge (right side).
View Figure 1
The ECG without ajmaline testing confirmed a QTc interval of 340 msec, what is per se the definition of short QT syndrome with the possible development of ventricular fibrillation and/or atrial fibrillation.
The ECG at rest and ajmaline challenge could identify four high risk parameters for the induction of ventricular fibrillation in Brugada syndrome:
Low amplitude type I Brugada ECG [1]
Localized right precordial QRS prolongation [2]
QRS fragmentation [3]
QTc interval of 340 msec or less [4]
After the diagnosis of early-stage arrhythmogenic cardiomyopathy and provocable Brugada ECG an intrathoracic defribrillator was implanted.
This case report combines four high risk markers for the development of ventricular fibrillation in Brugada syndrome at the early stage of arrhythmogenic cardiomyopathy with prehistologic abnormalities. In many cases ventricular fibrillation can be the first manifestation of arrhythmogenic cardiomyopathy as a pure electrical disease and later on manifest arrhythmogenic disease develops. It takes about 5 years to recurrent ventricular fibrillation according to a recent study [5]. In this period of time it is not an option to explant the ICD for missing arrhythmic events.