Different surgical approaches have been described for the treatment of maxillary atrophic alveolar ridges, such as the placement of short, angled implants or elevation of the Schneiderian membrane, highlighting within the latter the transcrestal approach, whose main associated concern is the risk of iatrogenic perforation of the sinus membrane due to limited access and indirect view of the procedure. In the literature, there are few studies reporting the use of 3D printed surgical guides for transcrestal flapless sinus membrane elevation. The objective of this study is to describe a surgical alternative for the immediate placement of implants in posterior maxillary bone height deficits, using a flapless guided transcrestal approach of the maxillary sinus through rotary instruments. Due to the prior planning of the surgical act through the use of CAD/CAM technology, this technique could provide greater safety to the clinician, reducing intraoperative risks and postoperative morbidity, as it is a minimally invasive procedure.
The use of osseointegrated implants is an efficient and reliable method for the long-term treatment of partially or fully edentulous patients. Premature loss of dental organs in the posterior maxillary sector is usually associated with alveolar ridge atrophy and increased degree of sinus pneumatization, resulting in reduced alveolar bone height, compromising conventional implant placement and constituting a clinical challenge for the oral and maxillofacial surgeon [1,2]. The presence of atrophic maxillary posterior alveolar ridges is the main indication for performing maxillary sinus floor elevations, since the presence of insufficient bone remnant compromises adequate implant stability [3].
Currently, there are two widely used techniques for sinus lift: Lateral and transcrestal approach, which have been shown to be the most stable techniques for vertical increase of bone tissue. In search of reducing postoperative morbidity and discomfort, Tamtun [4] in 1986 proposes the transcrestal approach through the sequential use of osteotomes to control the fracture of the maxillary sinus floor. In 2000, Cosci and Luccioli [5] proposed a transcrestal approach through the use of sequential elevation drills with a stopper to prevent perforation of the membrane. Thus, the transcrestal approach is defined as a conservative procedure compared to the lateral approach, however, its access and limited vision has been associated with intraoperative complications [6].
Implantology has advanced from conventional methods towards a more predictable therapy, which is why clinicians have sought to implement techniques that reduce surgical times, such as immediate implant placement, immediate loading or flapless approaches. The latter was introduced by Ledermann [7], in the late 1970s, to overcome the bone resorption process. Flapless surgery has been associated with less morbidity, resulting in less local trauma, used in conjunction with immediate implant placement in order to preserve blood supply and soft tissue contour [8].
Additionally, the use of three-dimensional images, implant planning software, CAD/CAM technology and guided surgery have led to modernization in implantology. This resources not only allow a successful preoperative evaluation but also facilitate the preoperative planning of the implant position through virtual placement of the implant and the subsequent transfer of the treatment plan to the patient, through the use of CAD/CAM, constituting a reliable element [9]. The purpose of this study is to present a case of the use of a surgical guide for transcrestal flapless maxillary sinus elevation and immediate placement of a dental implant.
A 50-year-old female patient attended to the Oral and Maxillofacial Surgery Unit of the University Hospital of Maracaibo, Venezuela with the chief complaint of an edentulous space in the right posterior maxillary region. Her medical record was unremarkable. Intraorally, absence of the upper right first molar was observed. On a panoramic X-ray, a limited osseous remnant with moderate atrophy in the aforementioned area was observed. A CBCT scan along with an extraoral scanning of the maxillary cast of the patient (Ceramill Map 300, Amann Girrbach, Austria) were obtained in order to get the DICOM and STL files respectively and the virtual planning was started using the Blue Sky Plan software (Blue Sky Bio, USA) to match both files and initiate the virtual implant placement. During this process, a 4.77 mm bone height was measured (Figure 1) and thus, a 4.5 × 7.3 mm implant was chosen for the case, in order to obtain primary anchorage in the remnant bone tissue, with the alternative of gaining approximately 3 mm of bone height through a transcrestal sinus floor elevation approach. After that, a surgical guide was designed and printed in a desktop 3D printer (Any Cubic Photon, China) (Figure 2). Under moderate sedation and local anesthesia, the surgical guide was placed and the drilling sequence was initiated through a flapless approach, 1 mm below the maxillary sinus floor. Through the use of rotary instruments, the elevation of the sinus membrane was performed until sufficient space was achieved using the Sinus Crestal Approach Kit (Neobiotech, Korea), in order to pack a combination of cortico-cancellous bone allograft (Ossogen, Lattice Biologics, USA) mixed with PRF made with Choukroun protocol. Subsequently, a 4.5 × 7.3 mm IS II implant was placed using the NeoBiotech Naviguide System (Neobiotech, Korea) obtaining a 35N cm torque. On the seventh postoperative day, the patient attended for checkup without signs of pain or swelling, with a healthy healing process of the area. A periapical X-ray was obtained at eighth postoperative week and the correct position, depth and angulation of the implant were observed (Figure 3).
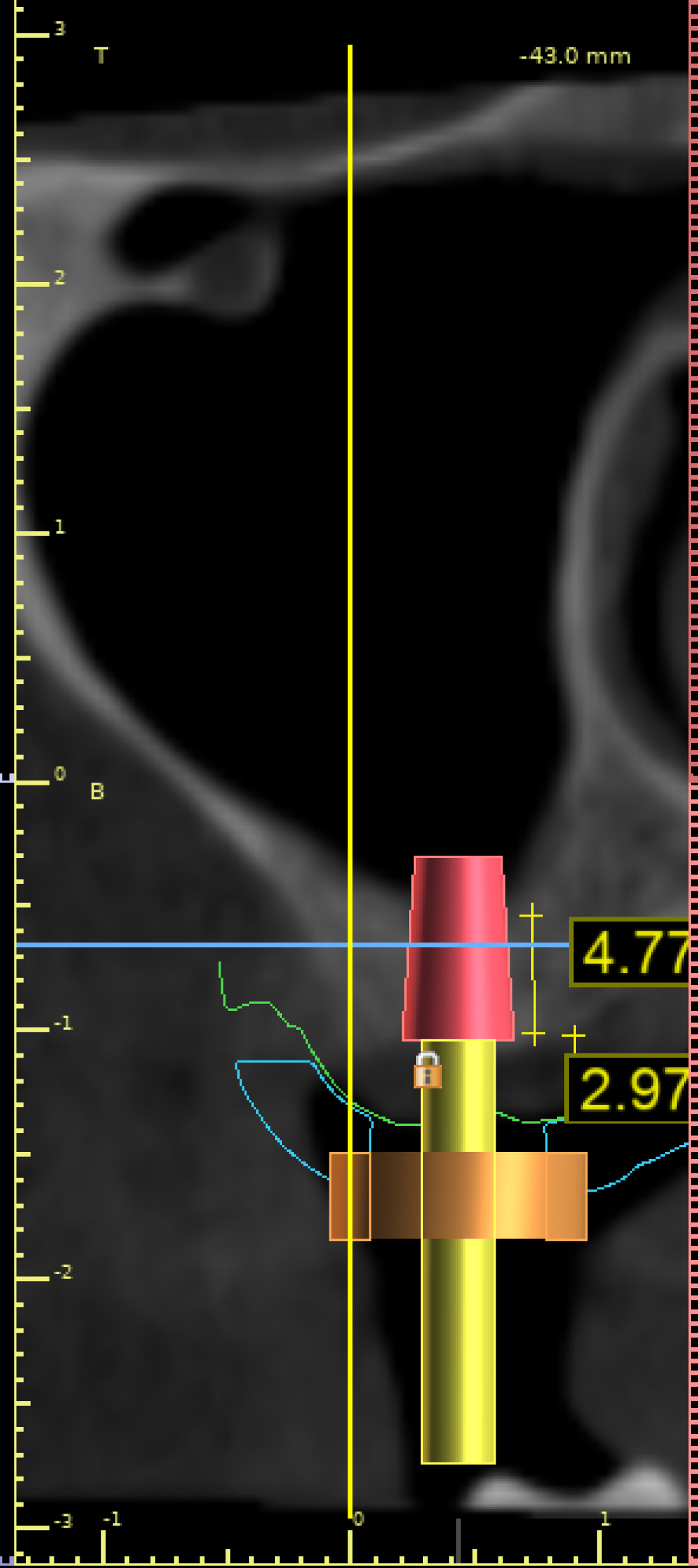 Figure 1: Bone height of 4.7 mm was measured during virtual planning and placement of the selected implant.
View Figure 1
Figure 1: Bone height of 4.7 mm was measured during virtual planning and placement of the selected implant.
View Figure 1
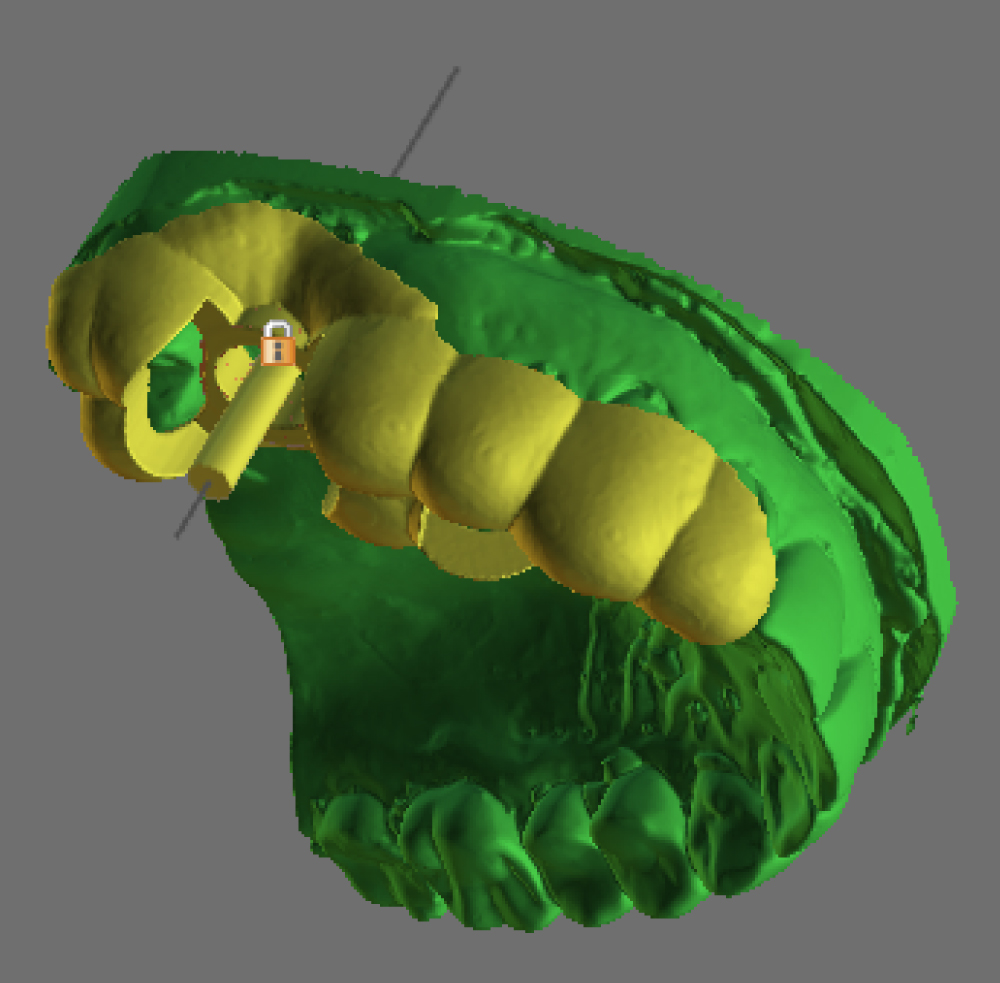 Figure 2: Virtual design of the surgical guide.
View Figure 2
Figure 2: Virtual design of the surgical guide.
View Figure 2
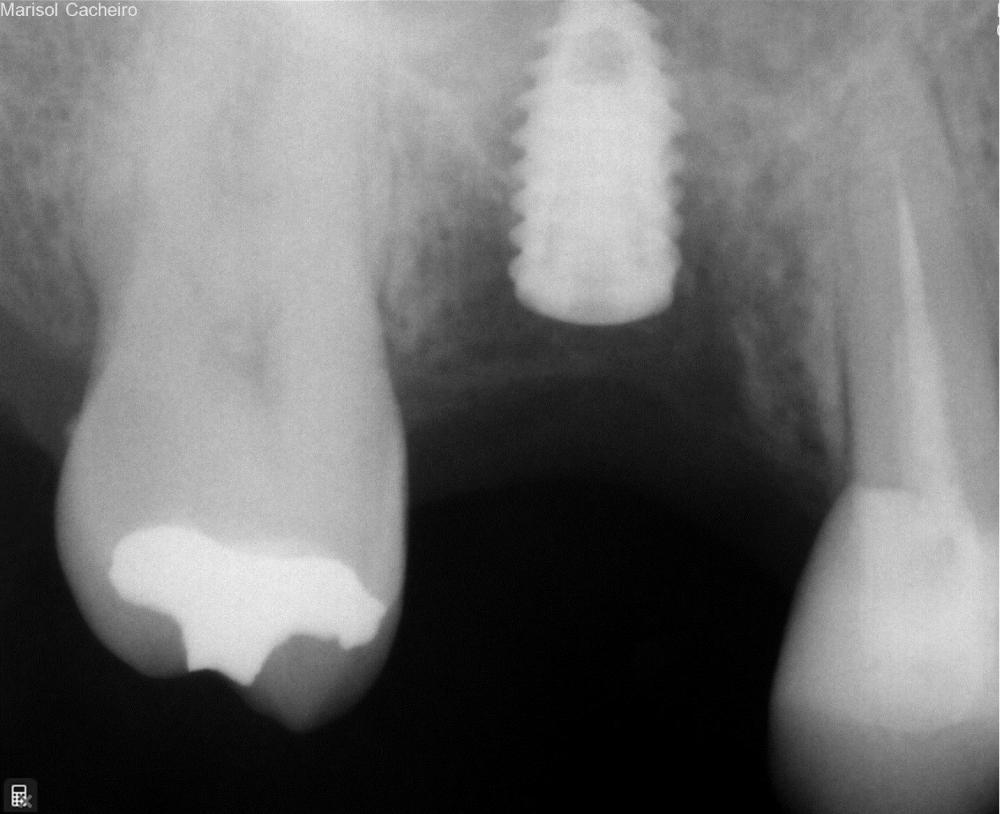 Figure 3: Eighth-week postoperative imaging of the implant.
View Figure 3
Figure 3: Eighth-week postoperative imaging of the implant.
View Figure 3
Maxillary sinus floor elevation is one of the approaches described to increase the amount of alveolar bone height, either by a lateral or a transcrestal technique. Pozzi, et al. described that although the transalveolar approach translates into less postoperative morbidity in contrast to the lateral antrostomy, the main concern associated with the technique is the fracture or perforation of the sinus membrane with the use of osteotomes or drills with or without stoppers, the indirect view of the sinus cavity, limited bone gain achieved and the high risk of inadvertent membrane perforation without the possibility of repair compared to the lateral approach [10].
Likewise, Chrcanovic, et al. mentioned that the flapless technique minimizes the possible loss of postoperative peri-implant tissue and overcomes the challenge of soft tissue management during or after surgery, however, among its possible complications, the risk of unwanted perforations is reported [11]. For this reason, the use of elements that reduce these complications is ideal, highlighting the use of guided surgery, which represents a minimally invasive technique, which in conjunction with the transcrestal procedure, prevents the need to make a flap with a minimum of intraoperative risks [10], associated with the prior planning of the surgical procedure through software and the confection of surgical guides, which allows greater control and safety when performing the elevation of the sinus membrane, as reported in our case.
In a retrospective study, Nasser, et al. evaluated the placement of 60 implants in 47 patients, using transcrestal sinus elevation, where they used rotating and calibrated drilling instruments with different lengths to achieve correct precision of the implant bed [12]. This protocol, like the one used in our case, allows lifting in an atraumatic, gradual and predictable way, preserving the Schneiderian membrane and allowing the introduction of the filling material.
Modern implant treatment requires systematic and controlled three-dimensional evaluation and planning. One of the most accepted methods worldwide is the use of digitally designed surgical guides, to guarantee an adequate and predictable long-term result; however, its success is strictly related to the surgeon's experience. In the literature review carried out for this study, there were no cases found where immediate implant placement would be performed using a guided flapless transcrestal approach to the maxillary sinus with rotary instruments, allograft and PRF; constituting a safe, conservative approach, with shorter surgical times and less intraoperative trauma, improving postoperative results for the patient. Based on the satisfactory results obtained, this protocol could be taken into account for the development of future research evaluating its success and long-term benefits compared to traditional techniques that allow immediate placement of implants in posterior alveolar atrophic ridges.
The University Hospital of Maracaibo IRB approved this study.
Patient's consent for publication was acquired.
Not applicable.
The authors declare that they have no competing interests.
No funding was received.
NS and PG participated as the main surgeons of the case. DO and AO participated as the prosthodontist of the case. NS, PG, DO and AP participated in the digital planning of the case. AP and ER participated in the drafting and editing of the article. All authors read and approved the final manuscript.
Not applicable.